Article Text

Abstract
Introduction Oesophageal and gastric cancer is common. Despite advances in investigation and treatment, the outcomes from these cancers remain poor. As part of the Be Clear On Cancer Campaign, the Department of Health runs the National Oesophagogastric Cancer Campaign each year, with key messages of (1) ‘Having heartburn most days, for 3 weeks or more could be a sign of cancer’ and (2) ‘if food is sticking when you swallow, tell your doctor’.
Methods We evaluated the effect of the National Oesophagogastric Cancer Campaign in our locality.
Results Reviewing new referrals from primary care for upper gastrointestinal symptoms during the campaign period, and a period thereafter, we found that there was no significant impact of the campaign in the diagnosis of oesophagogastric cancers. Furthermore, it increased routine waiting times for elective gastroscopies in our endoscopy units.
Conclusion We believe that alternative strategies need to be considered for earlier detection of oesophagogastric cancer.
- OESOPHAGEAL CANCER
- GASTRIC CANCER
Statistics from Altmetric.com
Introduction
Oesophageal and gastric cancers are the 13th and 16th most common cancers in the UK respectively, with over 7000 people diagnosed with oesophageal cancer and 6000 people with gastric cancer each year.1 The incidence of oesophageal cancer has steadily increased over the last decade, and it is the sixth most common cause of cancer death in the UK. The incidence of gastric cancer has decreased over time, most likely due to the improved detection and treatment of Helicobacter pylori infection. Despite this, the outcomes for these cancers remain poor, with a low 5-year survival of oesophageal and gastric cancer at 15% and 19%, respectively.1
At present, there is no screening programme for oesophagogastric cancers in the UK unlike a very successful Bowel Cancer Screening Programme to prevent colon cancers. To our knowledge, Japan is the only country that provides comprehensive screening for gastric cancer due to its high incidence in that country. Following the publication of the British Society of Gastroenterology (BSG) guidelines, surveillance endoscopy is recommended to patients with short-segment and long-segment Barrett's oesophagus (BO) with proven intestinal metaplasia.2 There is no rationale to screen all patients with gastro-oesophageal reflux disease for BO due to the low cancer transformation rate and the high costs associated with screening2
It is well known that for most cancers, outcomes are improved by an earlier diagnosis. Early oesophagogastric cancer which is limited to the mucosa is amenable to curative treatments either via endoscopic resection or radiofrequency ablation, thereby improving mortality. However, only a third of patients diagnosed with oesophagogastric cancers have early disease amenable to curative treatment; the remaining patients are unfortunately diagnosed late with advanced or metastatic disease, which is not curable. Prompt recognition of symptoms by family practitioners and timely investigation are key to earlier diagnosis. There are several strategies that could be used to achieve these, and they are based on modification of patient-related factors (raising awareness among the population to access healthcare professionals for symptoms), healthcare professional related factors (early referral for endoscopy) and service-related factors (rapid access to diagnostic endoscopy). In the UK, the demand for urgent endoscopies (referred to as the ‘2-week wait endoscopy’) is ever-increasing, resulting in a longer waiting period for non-urgent (routine) endoscopies. It would be important to identify patients who are at higher risk of malignancy, and therefore the need for prioritisation of investigations.
The Be Clear on Cancer Campaign is a Public Health England initiative to improve cancer outcomes by means of improving patient and primary healthcare provider awareness of signs and symptoms of early cancer. The specific campaign for oesophagogastric cancer ran from 26 January to 22 February 2015. This campaign carried two key messages—(1) ‘Having heartburn most days, for 3 weeks or more could be a sign of cancer’ and (2) ‘if food is sticking when you swallow, tell your doctor’. We analysed the impact of this cancer campaign in our locality of South Durham Hospitals to look at the direct gains of the campaign in terms of the diagnosis of oesophagogastric cancers and the impact of the campaign on the workload of our local endoscopy unit.
Methods
We collected data on all consecutive patients who were referred for an upper gastrointestinal (UGI) endoscopy for UGI symptoms. These patients were identified as additions to the elective gastroscopy waiting lists. The patients included were those newly referred from primary care for UGI tract symptoms such as dysphagia, dyspepsia, abdominal pain, nausea and vomiting. Referrals were classified into three categories: 2-week wait (2WW) referrals, urgent referrals and routine referrals. We excluded patients who were already known to secondary care physicians or surgical colleagues, patients who had a gastroscopy arranged following a recent hospital admission, patients who had their gastroscopy as inpatients, patients attending for variceal screening and those under surveillance for BO. We looked at two time periods, one to coincide with the oesophagogastric cancer campaign (February and March 2015), and a second period 4 months later, as a non-campaign period (June and July 2015).
After the exclusion criteria were applied, 406 patients were analysed across both periods. These included 283 patients during the campaign period (2WW––148, urgent––66, routine––69) and 123 patients during the non-campaign period (2WW––79, urgent––9, routine––35).
Results
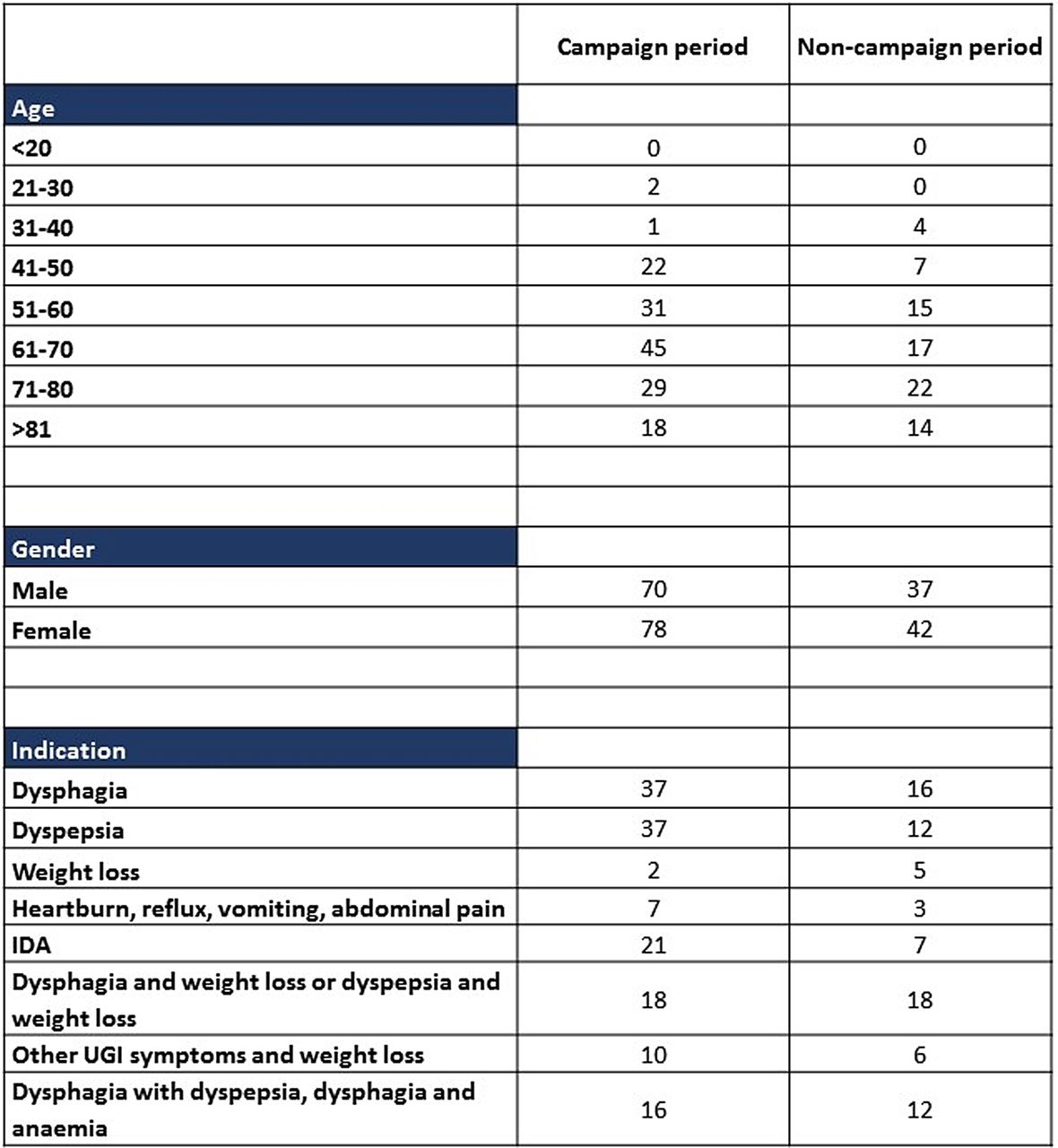
During the campaign period, the age group with the highest number of 2WW referrals was between 61 and 70 years, compared with 71–80 years for the non-campaign period. The gender distribution across both periods was similar. The most common symptom for referral was dysphagia or dyspepsia alone. Figure 1 shows the demographics of the cohort of patients referred as 2WWs.
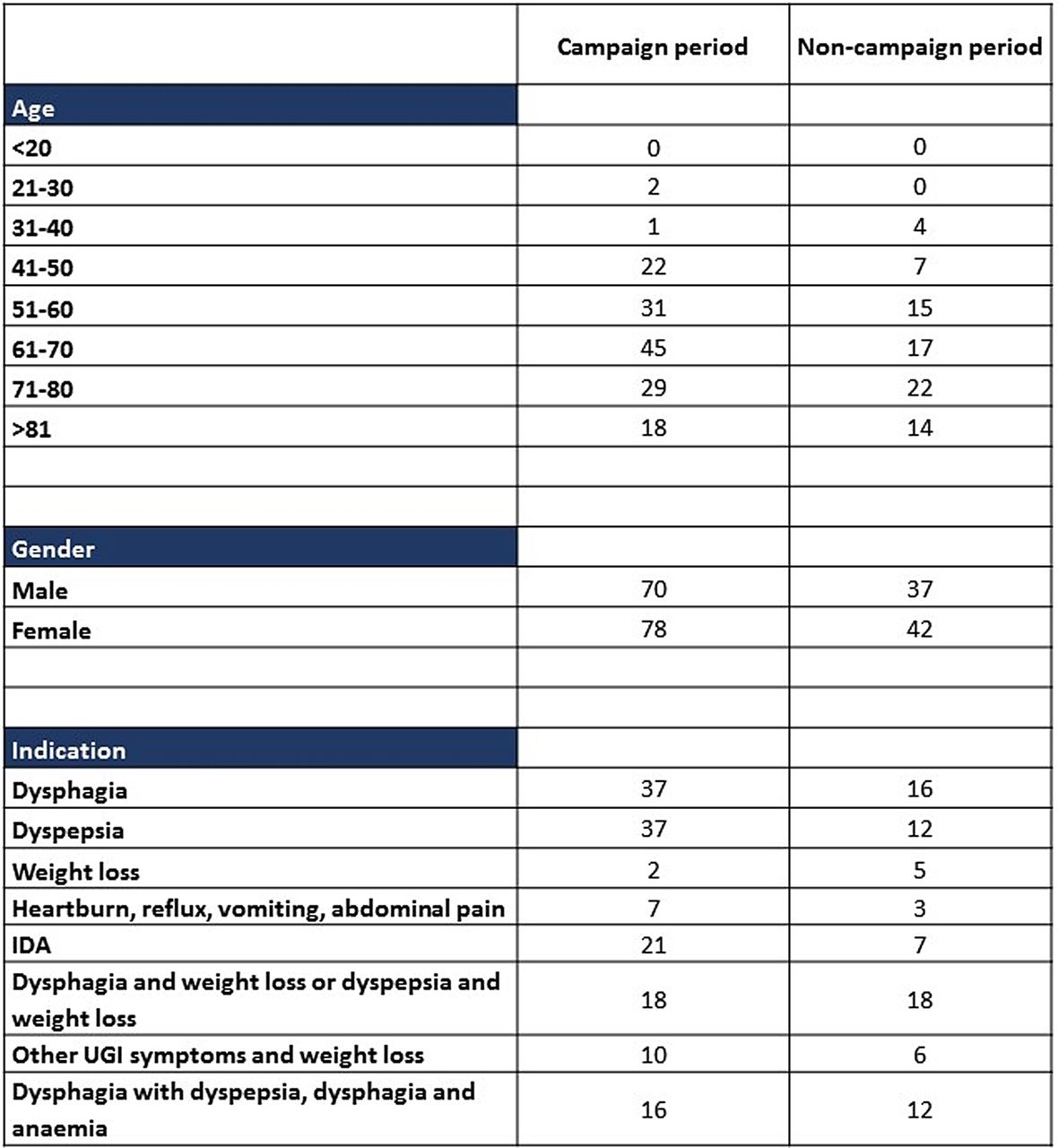
Demographic details and symptoms of patients referred under 2-week wait rule. UGI, upper gastrointestinal.
During the campaign period, two oesophagogastric cancers were detected, both within the 2WW referrals (1.35%). Both patients presented with dysphagia and weight loss. One patient was diagnosed with metastatic oesophageal squamous cell carcinoma and went on to receive palliative chemotherapy, but passed away shortly after diagnosis. The other patient was diagnosed with locally advanced gastric adenocarcinoma who declined palliative chemoradiotherapy.
During the non-campaign period, only one oesophagogastric cancer diagnosis was made in the 2WW referral group (1.27%). This patient presented with dyspepsia and weight loss, and was diagnosed with locally advanced gastric adenocarcinoma. The patient received palliative chemotherapy.
Interestingly, during the non-campaign period, two additional non-oesophagogastric cancers were diagnosed via 2WW referral. One patient was referred with dysphagia, and the gastroscopy revealed gastritis and previous gastrostomy but no oesophagogastric cancer. Subsequent investigation revealed metastatic adenocarcinoma of unknown primary on CT scanning. The other patient presented with anaemia, dyspepsia and weight loss. Gastroscopy revealed an irregular lesion on the lesser curve of stomach, and subsequent histological and cross-sectional imaging was consistent with a haematological malignancy. No oesophagogastric cancer diagnosis was made from urgent or routine referrals during both periods.
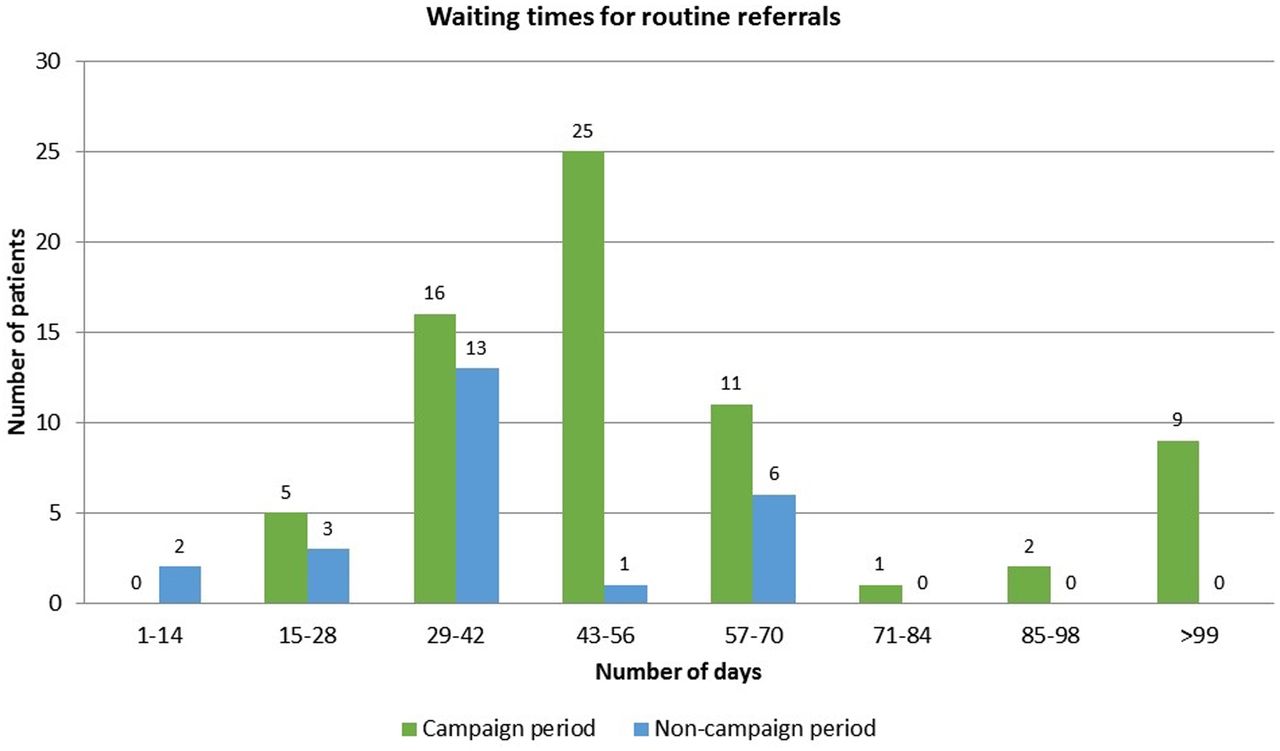
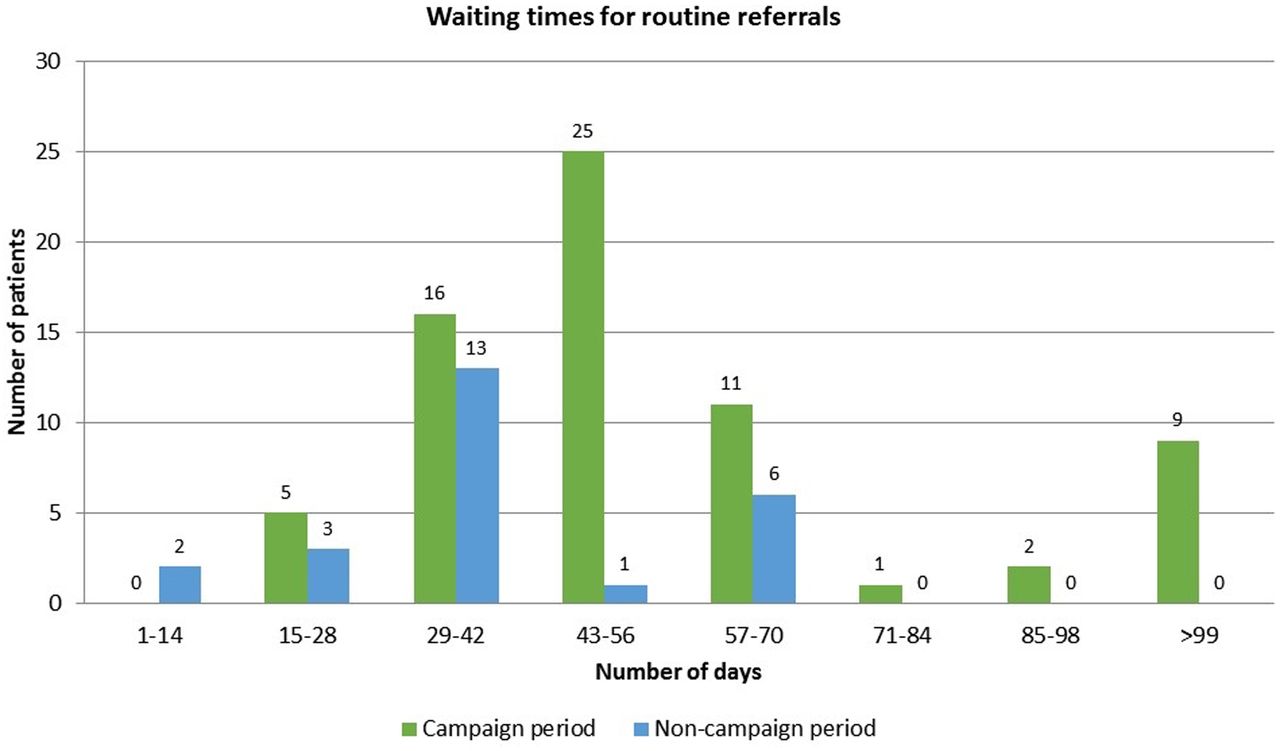
In terms of the impact of the campaign on endoscopy workload, the Oesophagogastric Cancer Awareness Campaign generated a significant increase in the numbers of endoscopy referrals by a factor of over 2, with little commensurate clinical gain of the intended outcome, that is, diagnosis of oesophagogastric (OG) cancer. This translated into an adverse impact on the waiting times for routine UGI endoscopy referrals. The increase in the number of 2WW referrals during the campaign period also resulted in an increase in median routine referral waiting times from an average of 29–42 days (during the non-campaign period) to 43–56 days during the campaign period (figure 2) The average waiting times for urgent referrals remained the same for both periods, at 29–42 days.
{kind=link}
{kind=link}
Waiting times for routine referrals.
Discussion
This report is the first locality analysis of the real impact and gains of a National Oesophagogastric Cancer Awareness Campaign. Unfortunately, the negative results of this analysis defeat the expectation that was intended with this campaign as part of the National Awareness and Early Diagnosis Initiative Campaign and the Saving 10 000 Lives Campaign. However, this study is quite important, as along with two other similar studies presented at the BSG meeting 2016, it highlights the need for a rethink about the national strategy for early diagnosis of oesophagogastric cancer.
In a large single-centre study of 1852 patients looking at the diagnosis of oesophagogastric cancers by 2WW referral, Kapoor et al3 found the yield of oesophagogastric cancer to be 3.8%. In our cohort, we found that despite the National Oesophagogastric Cancer Awareness Campaign, the clinical gain of a direct impact in increasing the OG cancer diagnosis is actually much lower (1.2%). One explanation for this might be that this campaign reflects a short intense period in the process of a longitudinal intervention to improve the awareness of both patients and healthcare providers of the need for early endoscopy referrals in patients presenting with UGI symptoms. There may also be a ‘lag phase’ phenomenon, whereby the desired impact of the campaign may only be felt after a longer period of the index campaign period.
Apart from iron deficiency anaemia, referrals for UGI endoscopy are largely based upon patient-reported symptoms. The difficulty is in differentiating patients at high risk of malignancy and those with significant non-malignant conditions. Clinical opinion in detecting malignancy is said to have a low sensitivity but high specificity. The current clinical practice is to investigate patients with alarm symptoms urgently, but these patients are more likely to have poorer outcomes due to advanced stages of disease leading to these alarm symptoms. Conversely, patients with early cancers are usually asymptomatic. At present, there is no validated risk-stratifying tool to aid clinicians in deciding upon the urgency of investigations for UGI symptoms.
There have been a number of studies that have looked at the correlation of UGI symptoms and oesophagogastric cancer diagnosis, with some studies reporting on the risk stratification of patients with UGI symptoms into a high-risk and a low-risk group. Purely relying on alarm symptoms is insufficient to detect malignancy, as <67% of patients diagnosed with cancer present with alarm symptoms.4 Kapoor et al3 have identified that of all alarm symptoms, dysphagia, weight loss and age above 55 years have significantly higher predictive value for a diagnosis of oesophagogastric cancer. Uncomplicated dyspepsia on the other hand has been found to be a negative predictor.3
Various studies have evaluated alarm symptoms in relation to cancer diagnosis in primary care. One such study by Stapley et al evaluated symptoms including dysphagia and dyspepsia. The authors found that in patients above 55, dyspepsia had a positive predictive value (PPV) of 0.7% for oesophagogastric cancer, but it is increased to 2.1% when it is present with weight loss.5 Dysphagia on the other hand has a PPV for oesophagogastric cancer at 4.8%, but increased to 9.8% if dysphagia was present with dyspepsia.5 Similarly, Jones et al6 found that the PPV of dysphagia for cancer was 5.3% in men and 2.1% in females. The common diagnoses in patients investigated for dysphagia include oesophagitis (7.1% in men, 5.4% in women), followed by hiatus hernia (4.6% in men, 4.8% in women).7 Oesophageal stricture was an uncommon finding for patients with dysphagia (2.9% of men and 1.7% of women).7 These studies illustrate the difficulty for primary care general physicians in teasing out patients truly at higher risk of malignancy with new UGI symptoms.
From a service provision viewpoint, any system that is being used to detect early cancer must have a high sensitivity and an affordable cost. However, improving current services by means of improving quality of gastroscopy and follow-up clinical care in the endoscopy unit should be a target of improvement. A study by Cheung et al8 in the UK revealed that the ‘missed’ UGI cancer rate among patients who had a gastroscopy in the preceding 12–36 months was 6.7%. This study also suggests that patients with recurrent reflux symptoms were three times more likely to have a malignancy compared with symptoms such as dysphagia. It has also been reported that the baseline referral pattern of GP practices also influences the detection of OG cancers, and patients with OG cancer belonging to practices with the lowest rates of gastroscopy referrals are at greatest risk of poor outcome arising out of late diagnosis and more advanced cancer.9 Although our study has not analysed the differential impact of an OG cancer campaign on the referral pattern of individual GP practices compared with the non-campaign period, it would be expected that the OG campaign would help in increasing the referrals from the low referring practices to improve cancer diagnosis. This has not been seen in the overall numbers of cancer diagnosed during the campaign period, and we therefore would conclude that the OG campaign does not remove this bias.
The present Oesophagogastric Cancer Awareness Campaign has generated higher number of referrals for endoscopy. There is also an associated increase in cost as gastroscopy is an expensive diagnostic investigation. Furthermore, with the increment in waiting times, this burden may exceed the capacity of some endoscopy units, thereby requiring outsourced endoscopy teams to meet the demand, further increasing cost. The campaign indicates the low sensitivity of the selection criterion for requesting an urgent 2WW endoscopy and suggests the need for a better risk assessment tool.
Conclusion
We believe that the positive impact of the National Oesophagogastric Cancer Awareness Campaign in increasing the number of oesophagogastric cancers is unlikely to be realised. Unlike other cancer awareness campaigns for lung cancer, bladder cancer and colorectal cancer, the poor symptom association of UGI symptoms with the diagnosis of oesophagogastric cancer is the main reason for this phenomenon. There is a significant adverse negative impact of the campaign on routine endoscopy waiting times, and the strain on endoscopy units lasts for several months following the campaign.
Significance of this study
What is already known on this topic?
A National Oesophagogastric Awareness Campaign may be able to detect patients with upper gastrointestinal symptoms, some of which may predict cancer, and selects them for appropriate diagnostic investigations such as an upper gastrointestinal endoscopy.
What this study adds?
This study for the first time shows that a single symptom criteria used in the National Oesophagogastric Cancer Awareness Campaign is unable to accurately detect patients who might have undiagnosed cancer, and hence a better set of symptoms together with a risk assessment tool may be needed to develop a cancer screening campaign for the upper digestive tract.
How might it impact on clinical practice in the foreseeable future?
The findings of this study together with similar locality analyses from other regions will help policy planners to fund future research into developing a upper GI risk assessment tool which may be able to better predict patients who are at higher risk of developing cancer, and this could be used to use diagnostic tools more cost-effectively.
Footnotes
Contributors AD conceptualised the study, reviewed the manuscript and stands guarantor for the accuracy of the research. SK collected and analysed the data and wrote the paper. BA collected the data.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.