Article Text

Abstract
Objective To gain an understanding of the efficacy of vedolizumab in a ‘real-world’ setting.
Design Retrospective cohort study using prospectively maintained clinical records.
Setting Two UK tertiary inflammatory bowel disease (IBD) centres.
Patients Patients with IBD commenced on vedolizumab at Guy's & St Thomas' and King's College Hospitals during November 2014–November 2015.
Intervention Vedolizumab, a monoclonal antibody to α-4 β-7 integrins that selectively inhibit leucocyte migration into the gut.
Main outcome measures Clinical disease activity was assessed at baseline, weeks 14 and 30 using Harvey–Bradshaw Index (HBI) for Crohn's disease (CD) and Simple Clinical Colitis Activity Index (SCCAI) for ulcerative colitis (UC). Response was defined as HBI or SCCAI reduction ≥3. Remission was defined as HBI <5 or SCCAI <3. Continuous data are summarised as medians, followed by range.
Results Fifty patients were included: 27 CD, 20 UC and 3 IBD-U (included in the UC group for analysis). At baseline visit, the median HBI was 8 (1–16) and SCCAI was 6 (0–15). At week 14, these values had fallen to 5 (0–15) (p=0.117) and 4 (0–10) (p=0.005), respectively. Additionally, week 30 data were available for 19 patients (9 CD, 10 UC). The clinical disease activity scores at that point were HBI 2 (0–7) (p=0.039) and SCCAI 2 (0–10) (p=0.023). At baseline, 37 (74%) of the 50 patients had clinically active disease. Of the patients with active disease, 22 (59%) responded and 14 (38%) achieved remission at week 14.
Conclusions Our early experience with vedolizumab demonstrates a clear benefit in terms of disease control as well as a steroid-sparing effect in a cohort, which included patients with complex and previously refractory disease.
- INFLAMMATORY BOWEL DISEASE
- CROHN'S DISEASE
- ULCERATIVE COLITIS
Statistics from Altmetric.com
Introduction
Crohn's disease (CD) and ulcerative colitis (UC) are chronic inflammatory conditions of the gut that are collectively referred to as inflammatory bowel disease (IBD). They are estimated to affect 240 000 people within the UK.1 The backbone of treatment for CD and moderate-to-severe UC are thiopurines, primarily azathioprine or mercaptopurine. However, these drugs are often poorly tolerated, associated with a number of side effects and a significant proportion of patients fail to achieve remission.2 This has led to the increased use of anti-tumour necrosis factor (anti-TNF) agents: infliximab, adalimumab and more recently golimumab. These drugs have proven efficacy3–7 but rates of non-response (primary or secondary) to anti-TNF agents are significant in both UC8 and CD.9 This, in addition to the risk of serious infection associated with TNF-blockade10 meant that there was an unmet medical need in the treatment of IBD.
Vedolizumab is a monoclonal antibody to α-4 β-7 integrins that selectively inhibit leucocyte migration into the gut. This offers an alternative mechanism of action to existing therapies. Large-scale, randomised, controlled trials have demonstrated efficacy in both UC (GEMINI 111) and CD (GEMINI 212). The reported rates of clinical remission after 1 year of vedolizumab treatment were 42% in UC and 39% in CD. In both cases, these were significantly greater than placebo-treated patients (16% and 22%, respectively).
Guy's and St. Thomas' Hospitals NHS Foundation Trust (GSTT) and King's College Hospital (KCH) are both tertiary IBD referral centres in South London. In 2014, the South East London IBD Pathway was created in collaboration with our local clinical commissioning groups (CCGs). Based on the proven efficacy seen in the GEMINI trials, this included approval of the use of vedolizumab from November 2014. This predated approval from the National Institute of Health and Care Excellence (NICE), which was subsequently granted in mid-2015. In both cases, the approvals were applicable to patients with moderate-to-severely active UC13 and patients with moderate-to-severely active CD14 who had previously failed anti-TNF therapy or where its use was considered inappropriate.
There is a growing appreciation of the importance of observational effectiveness research in IBD.15 Effectiveness relates to how well a treatment works in clinical practice, which is subtly (but importantly) different from efficacy, which relates to how well it works in clinical trials or laboratory studies.16 Due to our early access to vedolizumab and relatively large cohort of patients receiving treatment, we therefore had a desire to contribute to the growing body of existing observational data from the USA17–19 and Europe,20 ,21 which compliments knowledge gained from the GEMINI trials.
Methods
We performed a retrospective cohort study by reviewing prospectively maintained clinical records for all patients commencing vedolizumab at GSTT or KCH between November 2014 and November 2015. We screened the records of 62 patients, who received at least one infusion of vedolizumab for CD, UC or IBD-unclassified (IBD-U) during this data collection period. Patients who had not completed at least 14 weeks of treatment (n=5), had missing clinical disease activity data (n=2) or had a stoma (n=5) were excluded from further analysis. Of the five patients whose records were screened but had not reached 14 weeks of treatment, four had not started induction treatment 14 weeks prior to the data collection cut-off and one had discontinued prior to week 14 due to lack of non-response. Records of the remaining 50 patients were reviewed and patients with IBD-U (n=3) were included in the UC group for the purposes of analysis. Demographic information as well as the following disease-related data were collected: disease duration, distribution and behaviour (using the Montreal classification22), duration of vedolizumab treatment, prior anti-TNF exposure, concomitant immunomodulation and smoking status (table 1). We also collected data regarding how often we deemed it necessary to give an additional vedolizumab infusion at week 10, which is licensed in CD but not UC.
Baseline characteristics
Our primary outcome of interest was the clinical effectiveness of vedolizumab. This was evaluated by assessing clinical disease activity data at the following predefined time points: baseline (time of first vedolizumab infusion), week 14 and week 30, where available (figure 1). At each time point, clinical disease activity was evaluated using the Harvey–Bradshaw Index23 (HBI) for CD and the Simple Clinical Colitis Activity Index24 (SCCAI) for UC. Treatment outcomes were predefined as follows: clinical response was defined as a reduction of three or more in HBI or SCCAI, clinical remission was defined as HBI <5 or SCCAI <3. These definitions were based on their previously demonstrated (partial) validity25 ,26 and published post-marketing experiences of vedolizumab in an attempt to aid comparability of results.17 ,19

Study design and evaluations (VDZ, vedolizumab; CRP; C reactive protein; FC, faecal calprotectin; HBI, Harvey–Bradshaw Index; SCCAI, Simple Clinical Colitis Index; *optional, additional week 10 dose in Crohn's disease (CD)).
Secondary outcomes included the effect of vedolizumab on biochemical markers of disease activity, rates of corticosteroid use and the need for IBD-related abdominal surgery. At each study time point, biochemical disease activity was assessed using serum C reactive protein (CRP) measurements. A level of 5 mg/L or greater was considered biochemical evidence of disease activity. In addition, where available pre-treatment and post-treatment faecal calprotectin (FC) measurements were included. A FC value of <150 µg/g was considered indicative of biochemical remission.27 Rates of corticosteroid (prednisone or budesonide) usage at each time point were also collected. IBD-related surgery was included in our outcome assessments if it occurred within 30 weeks of vedolizumab initiation.
Continuous data are summarised as medians and range. Paired HBI, SCCAI, CRP and FC values were compared using Wilcoxon signed-rank test. Categorical variables were compared using the Fisher's exact test (GraphPad Prism V.7.0a). Unless stated, p values are non-significant.
Results
Clinical disease activity
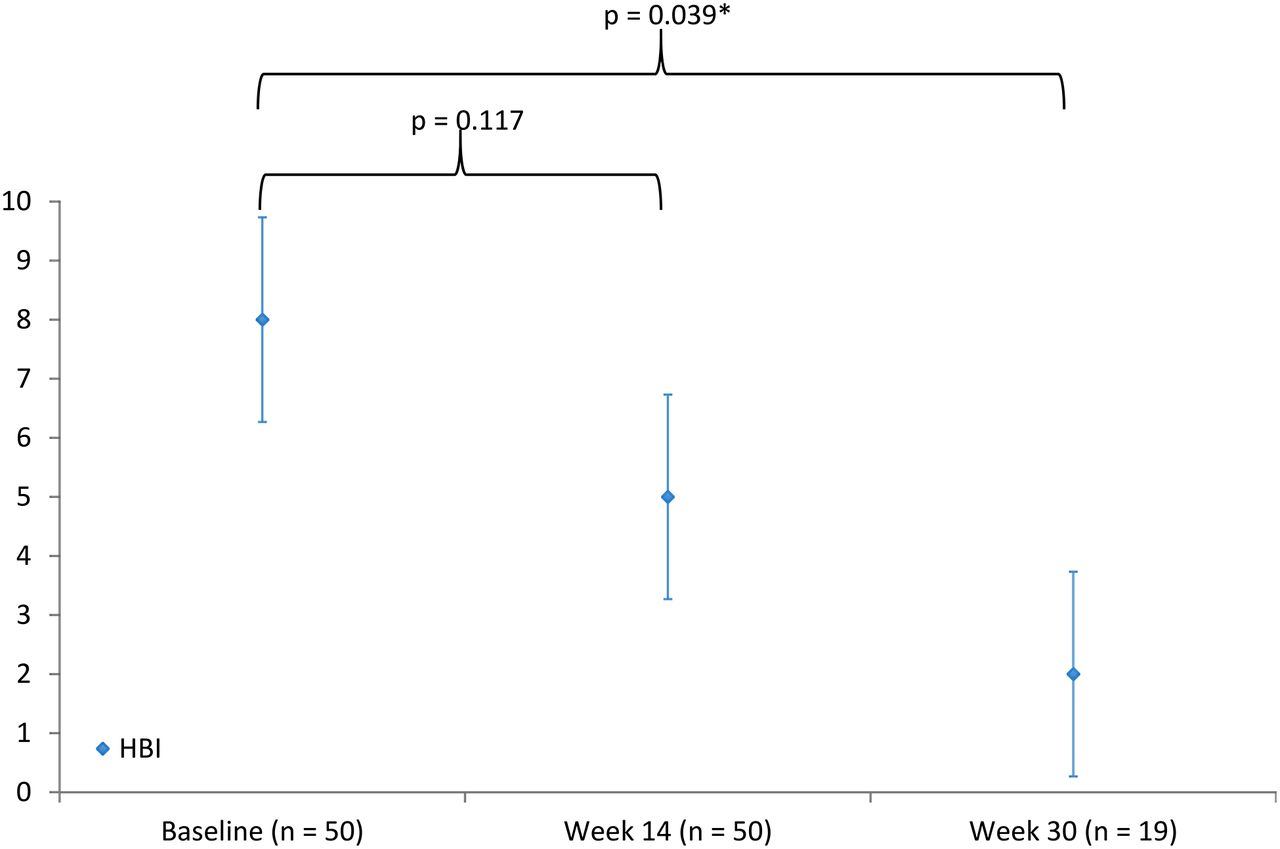
At the baseline visit, the median HBI was 8 (range 1–16) and SCCAI was 6 (range 0–15). Week 14 scores were available for all 50 patients, by which time these values had fallen to 5 (0–15) (p=0.117) and 4 (0–10) (p=0.005), respectively (figures 2 and 3).

Median Simple Clinical Colitis Index (SCCAI) at each study time point (NB: week 30 analysis only includes the subgroup of patients reaching this time point and excludes two patients who stopped treatment prematurely due to non-response).

Median Harvey–Bradshaw Index (HBI) at each study time point (NB: week 30 analysis only includes the subgroup of patients reaching this time point and excludes four patients who stopped treatment prematurely due to non-response).
Response and remission at week 14
At baseline, 37 (74%) of the 50 patients had clinically active disease (HBI ≥5, SCCAI ≥3). Of the patients with active disease, 22 (59%) responded of whom 14 (38%) achieved remission. Divided by IBD subtype, response rates were 12/19 (63%) in CD and 10/18 (55%) in UC. Remission rates were 7/19 (37%) in CD and 7/18 (39%) in UC (figure 4).

Week 14 response, remission and corticosteroid-free remission rates among patients with UC and Crohn's disease (CD) with active disease at baseline. Response defined as Harvey–Bradshaw Index (HBI) or Simple Clinical Colitis Activity Index (SCCAI) reduction ≥3. Remission defined as HBI <5 or SCCAI <3.
Divided by prior anti-TNF exposure, response rates were 5/8 (63%) in anti-TNF naïve and 17/29 (59%) in anti-TNF exposed patients. Corresponding remission rates were 5/8 (63%) and 9/29 (33%), respectively (figure 5). Dividing patients by those receiving vedolizumab monotherapy or in combination with an immunomodulator, the response rates were 13/21 (62%) and 9/16 (56%), respectively. The rates of remission were 6/21 (29%) for monotherapy and 8/16 (50%) for combo therapy. Dividing patients with CD by disease location, the following rates of response and remission were observed: ileal: 3/4 (75%), 1/4 (25%); colonic: 6/9 (64%), 5/9 (56%); and ileocolonic: 3/6 (50%), 1/6 (17%).

Week 14 response and remission rates among anti-tumour necrosis factor (anti-TNF) exposed and naïve patients with active disease at baseline. Response defined as Harvey–Bradshaw Index (HBI) or Simple Clinical Colitis Activity Index (SCCAI) reduction ≥3. Remission defined as HBI <5 or SCCAI <3.
Of the 13 patients with inactive clinical disease at baseline, 8 (62%) remained in remission at week 14. Seven of these 13 patients (54%) were receiving steroid treatment at baseline, of whom 2 were able to cease steroids by week 14. Indications for commencing vedolizumab in these patients included steroid dependency and/or active disease demonstrated endoscopically or radiologically.
Response and remission at week 30
Week 30 data were available for 19 patients (9 CD and 10 UC). The median clinical disease activity scores at that point were HBI 2 (0–7) and SCCAI 2 (1–10), reflecting a significant fall from baseline values and remission in both conditions (p=0.039 and 0.023, respectively). Of the 31 patients who did not have week 30 follow-up data: 24 had not started induction treatment 30 weeks prior to the data collection cut-off, 6 stopped due to non-response (4 of whom underwent surgery) and 1 patient (a week 14 responder) stopped due to intolerance (dizziness and headaches). Fourteen (6 CD and 8 UC) of the patients completing 30 weeks of treatment had active disease at baseline. So too, did the six (4 CD and 2 UC) non-responders who did not complete 30 weeks, whose data were carried forward to the week 30 time point for the purposes of analysis. The overall rate of response was 11/20 (55%) with 10/20 (50%) achieving remission. Dividing by IBD subtype, the response rate was 5/10 (50%) for CD and 6/10 (60%) for UC. Corresponding remission rates were 5/10 (50%) in CD and 5/10 (50%) in UC.
Biochemical disease activity
Serum CRP data were available for 49 patients at baseline and week 14, with additional week 30 data for 19 patients. The median baseline result was 4 (1–70) mg/L and this remained unchanged at week 14 (1–72) and week 30 (1–80). Twenty-three of the 49 patients (47%) had an elevated CRP (≥5 mg/L) at baseline (14 CD and 9 UC). Of the 23 patients with an elevated baseline CRP, a fall was observed in 15/23 (65%) and normalisation (<5 mg/L) in 8/23 (35%), after 14 weeks of treatment.
The median baseline CRP among patients with CD was 7 mg/L, falling to 5 mg/L at week 14. The median CRP among patients with UC was 3 mg/L at baseline and 2 mg/L at week 14.
Paired pretreatment and post-week 14 FC data were available for 18 patients. FC fell significantly between these two time points from 1076 µg/g (27–4800) to 476 µg/g (10–3184) (p=0.010). Sixteen of these 18 patients (89%) had an elevated (≥150 µg/g) FC at baseline (6 CD and 10 UC). Of the 16 patients with an elevated baseline FC, a fall was observed in 13/16 (81%) and normalisation (<150 µg/g) in 5/16 (31%), after 14 weeks of treatment.
Corticosteroid usage and surgery rates
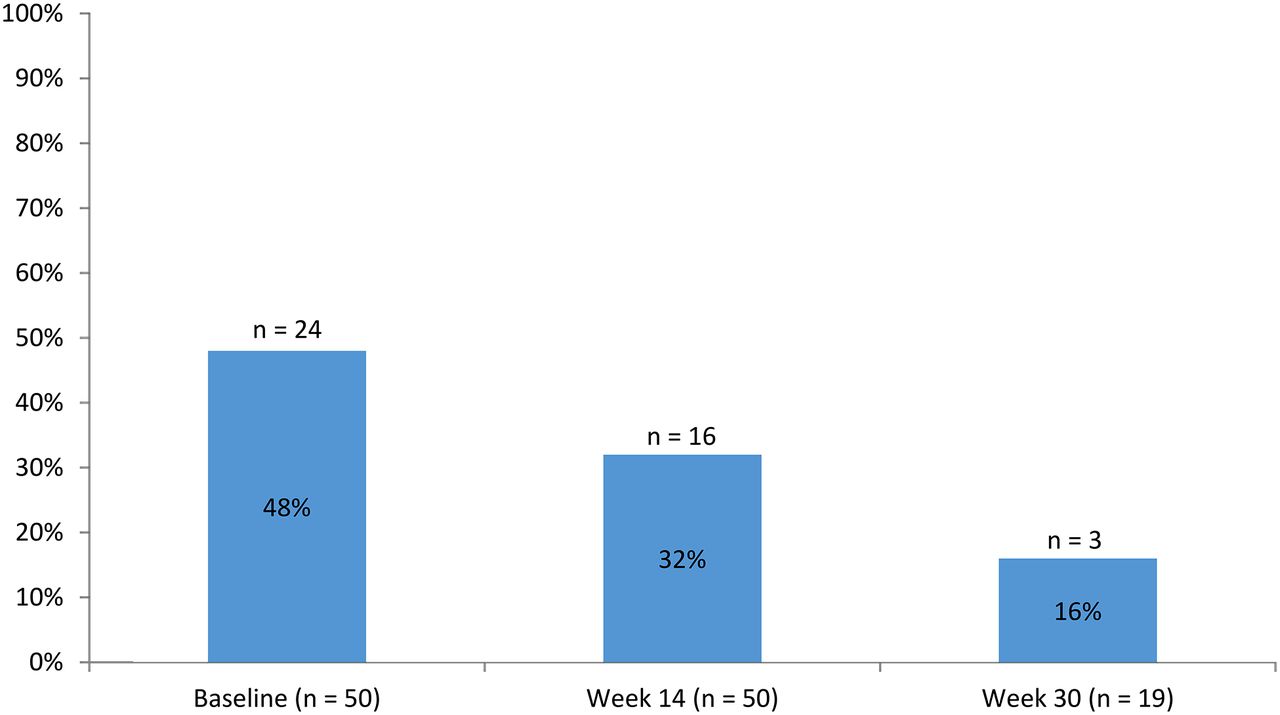
At baseline, 24/50 (48%) patients were receiving corticosteroid treatment. This number had fallen to 16/50 (32%) by week 14 and reduced further to 3/19 (16%) by week 30 (p=0.008) (figure 6). The rates of corticosteroid-free remission (UC and CD combined) at those time points were 11/37 (30%) and 9/14 (64%), respectively (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rates of corticosteroid usage at each study time point.
Four (8%) patients (three CD and one UC) who failed to respond to vedolizumab required surgery within 30 weeks of commencing treatment.
Discussion
The results of our study closely resemble those seen in large-scale, randomised, placebo controlled trials11 ,12 as well as previously reported ‘real-world’ cohorts19–21 from the USA and Europe. Patients in our cohort had a similar duration of disease and rates of corticosteroid usage to those seen in the GEMINI trials. However, our cohort had a higher rate of prior anti-TNF exposure (76% in our cohort vs 48% in GEMINI 1 and 62% in GEMINI 2). This finding reflects current patterns of practice, particularly in CD, in which anti-TNF agents are generally used as first-line biological agents unless contraindications such as infective or malignant concerns exist. Indeed, the rate of prior anti-TNF exposure was as high as 87% in the Chicago cohort19 and higher still in the cohort recently reported by GETAID (Groupe d'Etude Therapeutique des Affections Inflammatoires du tube Digestif), with 99% of CD and 98% of patients with UC having previous exposure.20 These findings serve to demonstrate the refractory nature of the patients encountered at tertiary IBD referral centres. In addition, our cohort included patients with considerably active disease at baseline; our median HBI of 8 and SCCAI of 6 were compared with 5.8 and 4.5, respectively, in the Chicago cohort. Our baseline median FC was also considerably elevated when compared with the GEMINI trials (1072 µg/g vs 899 µg/g in GEMINI 1 and 686 µg/g in GEMINI 2). However, FC data reported in the only other observational study to collect FC data were higher still (975 µg/g in CD and 1740 µg/g in UC).21 CRP values were not reported in GEMINI 1 but they were in GEMINI 2, presumably because CRP correlates less well with disease activity in UC than CD. The median baseline CRP in GEMINI 2 was 11.5 mg/L, which compares with 7 mg/L in our CD cohort. The GEMINI 2 authors defined an elevated CRP as >2.87 mg/L, with 83.2% of patients having an elevated value at baseline. Using their definition for an elevated CRP (rather than our own arbitrary definition of 5 mg/L), 22 out of 27 (81%) of the patients with CD in our cohort had an elevated value at baseline.
Despite the active and refractory nature of the disease in this cohort, we observed a fall in disease activity after 14 weeks of treatment, which allowed a substantial proportion of patients (38%) to enter remission. Moreover, this benefit was demonstrated to increase in patients who continued maintenance therapy out to 30 weeks (50% remission). This finding serves to underscore the seemingly rather gradual onset of action of vedolizumab. This observation is relevant to practice and should encourage clinicians to allow sufficient time before drawing conclusions regarding treatment success or failure. Week 14 seems a reasonable, pragmatic and increasingly evidence-based time point to make this assessment.18 In the absence of a signal of clinical efficacy at that point, objective markers of disease activity should be sought and alternative treatment options should be considered. Ideally, where possible these options should be considered in the setting of a dedicated multidisciplinary biologics meeting. However, where a signal is recognised, our data would suggest that treatment continuation has a good chance of delivering either remission, or failing that, a maintained response. Our study showed that vedolizumab allowed steroid weaning in a significant proportion of patients, an important treatment goal for patients and clinicians alike. However, it is also important to consider that many patients benefit from concomitant steroid use during the induction phase as a way of controlling their symptoms while waiting for an effect of vedolizumab.
We did not observe a difference in treatment outcomes between patients with UC and CD, but there was a trend to their being a difference based on prior anti-TNF exposure. Although the exact reason for anti-TNF cessation in our cohort is not known (failure vs adverse effects), several possible explanations for this difference exist and are the subject of great interest. Assuming the majority of anti-TNF-exposed patients had previously failed treatment, it is possible that their disease is simply more refractory and may be more difficult to control pharmacologically, whatever mode of action is employed. Alternatively (and perhaps more intriguingly), there is the possibility that prior anti-TNF exposure (independent of the reason for cessation) alters the biology of the disease and renders the inflammation less responsive to treatment with vedolizumab. This is certainly a matter that requires dedicated basic science research for elucidation. However, a direct head-to-head trial of the comparative effectiveness of anti-TNF (infliximab) versus selective leucocyte adhesion molecule inhibition (etrolizumab, which has a similar mechanism to vedolizumab) is ongoing and may also be informative in this regard.28
The choice of mechanism for first-line biological treatment is certainly a current ‘hot-topic’ for debate but in lieu of clear randomised controlled trial evidence to settle the matter; our practice is to discuss each case in a multidisciplinary setting. The appropriate choice and management of biological drugs (eg, deciding when to administer the optional week 10 vedolizumab dose in CD) is often a matter of nuance that incorporates multiple factors, best addressed by physicians with an specialist interest in IBD as well as IBD Clinical Nurse Specialists. We, therefore, discuss all relevant aspects of cases where a biological is being considered as part of a weekly virtual biologics and immunosuppressives clinic (VBIC). This includes IBD-specific factors such as the predominance of extraintestinal manifestations or perianal disease (where anti-TNF may be preferred) as well as medical comorbidities such as predisposition or history of malignancy or infection (where vedolizumab may be preferred). In addition, practical factors such as patient preference for route of administration and the management of pressures on infusion suite capacity should be considered. It should be appreciated that this is a rapidly moving field and that the next wave of biologic (eg, ustekinumab and etrolizumab) and small molecule (eg, tofacitinib and ozanimod) drugs will add further complexity.
Our study has several limitations. Most notable are its retrospective design and the subjective nature of the clinical disease activity scores employed. In addition, other than rates of surgery, we did not have systematically collected data regarding adverse events. Although our CRP data were almost entirely complete, we had paired, pretreatment and posttreatment FC data on only a limited number of patients. Even with these limited data, FC seemed to outperform CRP, both in terms of indicating disease activity and being responsive to change induced by vedolizumab. It would also have been preferable to have week 30 data on all subjects. Endoscopic outcomes would also have been of interest although these data were only sparsely available in this cohort. Finally, the presented high rates of response and remission at week 30 should be interpreted in the context of a ‘per-protocol’ analysis in which patients who failed to respond (eg, and required surgery) were less likely to continue treatment at this time point.
Nonetheless, despite these limitations we believe the results generated in our study are relevant, reliable and generalisable. Indeed, this type of observational effectiveness research is becoming increasingly recognised as significant and necessary.15
Conclusion
Our early experience with vedolizumab in two tertiary IBD centres mirrors the efficacy data seen in a previous, real-world cohort as well as the GEMINI trial programme. Our data demonstrate a clear benefit in terms of disease control as well as a steroid-sparing effect in a cohort that included patients with complex and previously refractory disease. Outcomes appeared more favourable among anti-TNF naïve patients than those with previous exposure but did not differ between UC and CD.
Significant of this study
What is already known on this topic?
The GEMINI trials demonstrated the efficacy of vedolizumab for both ulcerative colitis (UC) and Crohn's disease (CD).
The treatment effect size observed in the GEMINI trials was greater among anti-tumour necrosis factor (anti-TNF) naïve patients than those previously exposed to anti-TNF agents.
What this study adds?
Our data demonstrate the efficacy of vedolizumab in a ‘real-world’ cohort of complex and previously treated patients with refractory inflammatory bowel disease (IBD).
Our findings suggest vedolizumab has similar effectiveness in achieving a clinical response in CD and UC.
How might it impact on clinical practice in the foreseeable future?
Clinicians should consider vedolizumab in patients with UC or CD failing conventional therapies as well as patients who are steroid dependent.
Clinicians and their patients should be aware of the somewhat gradual and incremental beneficial effect of vedolizumab, meaning that responders may expect further improvement in clinical disease activity beyond week 14 of treatment.
References
Footnotes
Contributors MAS, PP, EJ, BW, JD-B, IK, JB-S, B'HH and PMI were responsible for the original concept and planning of the study. MAS, PP, EJ, BW, JD-B, IK, SF, RG, KP, SG, LM, MS, CB-C, JB-S, KF, EL, AS and JD were responsible for data collection and analysis. MAS, PP and EJ drafted the manuscript, which GC-F, PD, NP, SA, JS, B’HH and PMI critically reviewed and revised.
Competing interests MAS Advisory board: Hospira Lecturing and training: Hospira, Takeda, MSD. JD lectures and/or consultant for Abbvie, MSD, Allergan, Dr Falk Pharma and Takeda. PMI Lecture fees: Abbvie, Warner Chilcott, Ferring, Falk Pharma, Takeda, MSD, Johnson and Johnson, Shire. Financial support for research: MSD and Takeda. Advisory fees: Abbvie, Warner Chilcott, Takeda, MSD, Vifor Pharma, Pharmacosmos, Topivert, Genentech, Hospira and Samsung Bioepis.
Ethics approval The Health Research Authority does not consider postmarketing surveillance research and therefore suggests that NHS REC approval is not necessary for our study.
Provenance and peer review Not commissioned; externally peer reviewed.