Article Text

Abstract
Patient safety incidents occur throughout healthcare and early reports have exposed how deficiencies in ‘human factors’ have contributed to mortality in endoscopy. Recognising this, in the UK, the Joint Advisory Group for Gastrointestinal Endoscopy have implemented a number of initiatives including the ‘Improving Safety and Reducing Error in Endoscopy’ (ISREE) strategy. Within this, simulation training in human factors and Endoscopic Non-Technical Skills (ENTS) is being developed. Across healthcare, simulation training has been shown to improve team skills and patient outcomes. Although the literature is sparse, integrated and in situ simulation modalities have shown promise in endoscopy. Outcomes demonstrate improved individual and team performance and development of skills that aid clinical practice. Additionally, the use of simulation training to detect latent errors in the working environment is of significant value in reducing error and preventing harm. Implementation of simulation training at local and regional levels can be successfully achieved with collaboration between organisational, educational and clinical leads. Nationally, simulation strategies are a key aspect of the ISREE strategy to improve ENTS training. These may include integration of simulation into current training or development of novel simulation-based curricula. However used, it is evident that simulation training is an important tool in developing safer endoscopy.
- endoscopy
Statistics from Altmetric.com
Introduction
Medical error or patient safety incidents (PSIs) occur throughout all branches of medicine.1 The 2004 ‘National Confidential Enquiry into Patient Outcomes and Death’ (NCEPOD) report estimated a 3% inpatient 30-day mortality rate after therapeutic endoscopy.2 The report highlighted deficiencies in non-technical skills (NTS) as contributory but the extent of their influence was unclear. The authors of a recent systematic literature review concluded that NTS are an ‘essential component’ of endoscopic practice.3
The Joint Advisory Group for Gastrointestinal Endoscopy (JAG) has developed several initiatives to promote safer endoscopy. The Global Rating Scale (GRS) rates endoscopy units in terms of clinical quality, patient experience, workforce and training,4 in order to drive improvements in care. The implementation of safety checklists has improved the processes around endoscopy, aiming to reduce error and improve teamworking.5 Demonstrating the impact of JAG initiatives on safety is challenging. Nevertheless, a recent literature review of 34 studies highlighted how initiatives may contribute to improved quality of care through safer sedation, improved patient comfort and lower risk of post-colonoscopy colorectal carcinoma.6
It is apparent that the nature of endoscopy is changing. A recent nationwide survey identified the significantly increasing demand and lack of capacity in endoscopy.7 Together with increasingly therapeutic and complex procedures, these pressures will inevitably play a role in the quality and safety of endoscopy.8
Training and assessment have been crucial in improving safety. The implementation of an e-portfolio, mandated training courses and validated assessment have led to a significant improvement in endoscopic training in the UK over the last two decades. The recent introduction of the Endoscopic Non-Technical Skills (ENTS) framework into Direct Observation of Procedural Skills (DOPS) reflects the acknowledgement of the impact of ENTS on safety in endoscopy.9
What is ISREE?
Recognising the ongoing need to understand and improve safety in endoscopy, JAG has recently developed the ‘Improving Safety and Reducing Error in Endoscopy’ (ISREE) implementation strategy.10 Key strategic aims are outlined below:
Improving training in ENTS and incident reporting.
Promoting measures to prevent PSIs.
Promoting PSI reporting.
Promoting learning from incidents.
Supporting underperforming services/endoscopists.
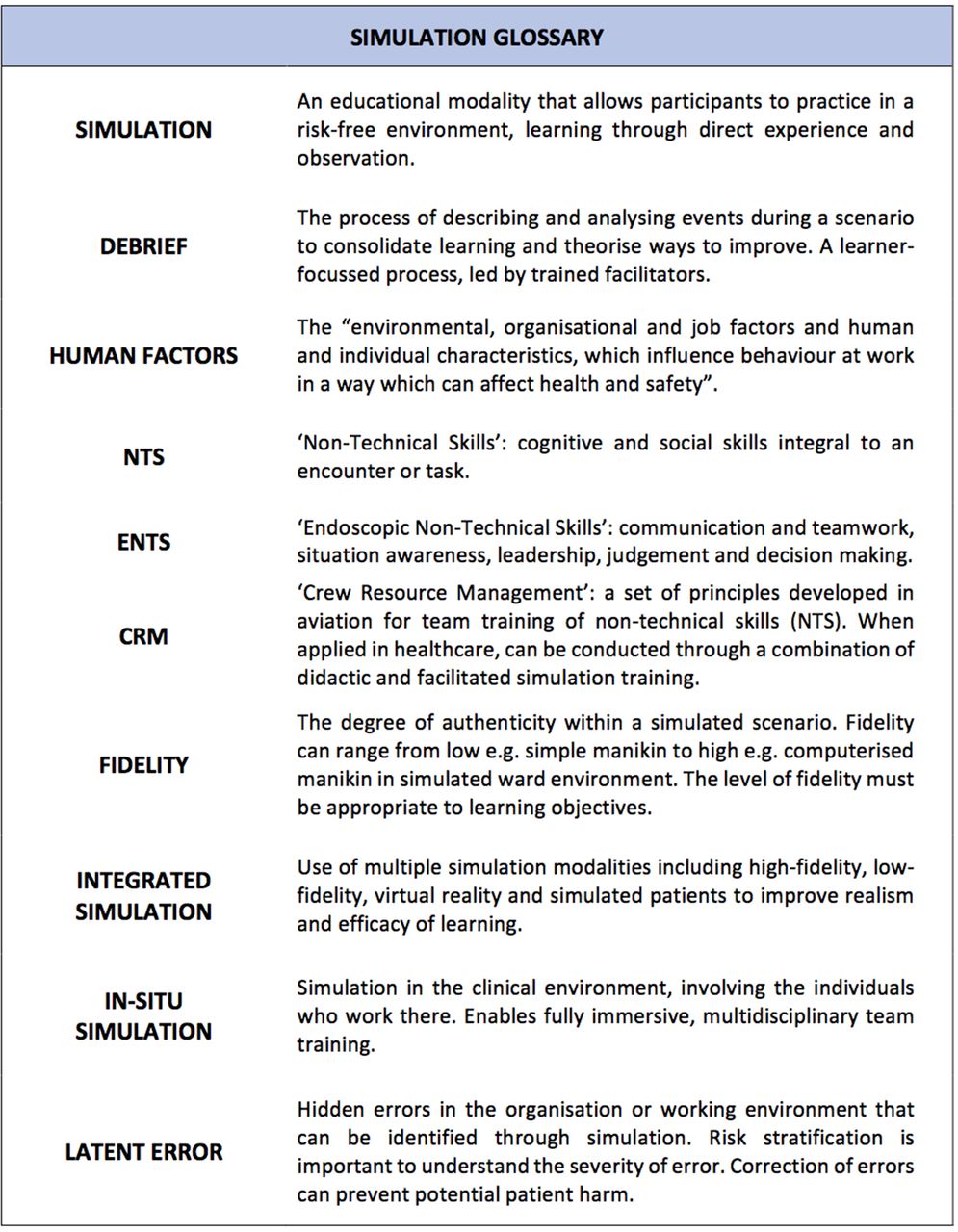
The JAG Quality Assurance of Training (QA-T) group acknowledges that, although no national ENTS training currently exists, certain training strategies may be of use. The group have identified simulation as an educational modality of interest in this setting. The aim of this article is to highlight the use of simulation to develop ENTS training in promoting safer endoscopy. For reference, a glossary of terms related to simulation training in endoscopy is shown in figure 1.
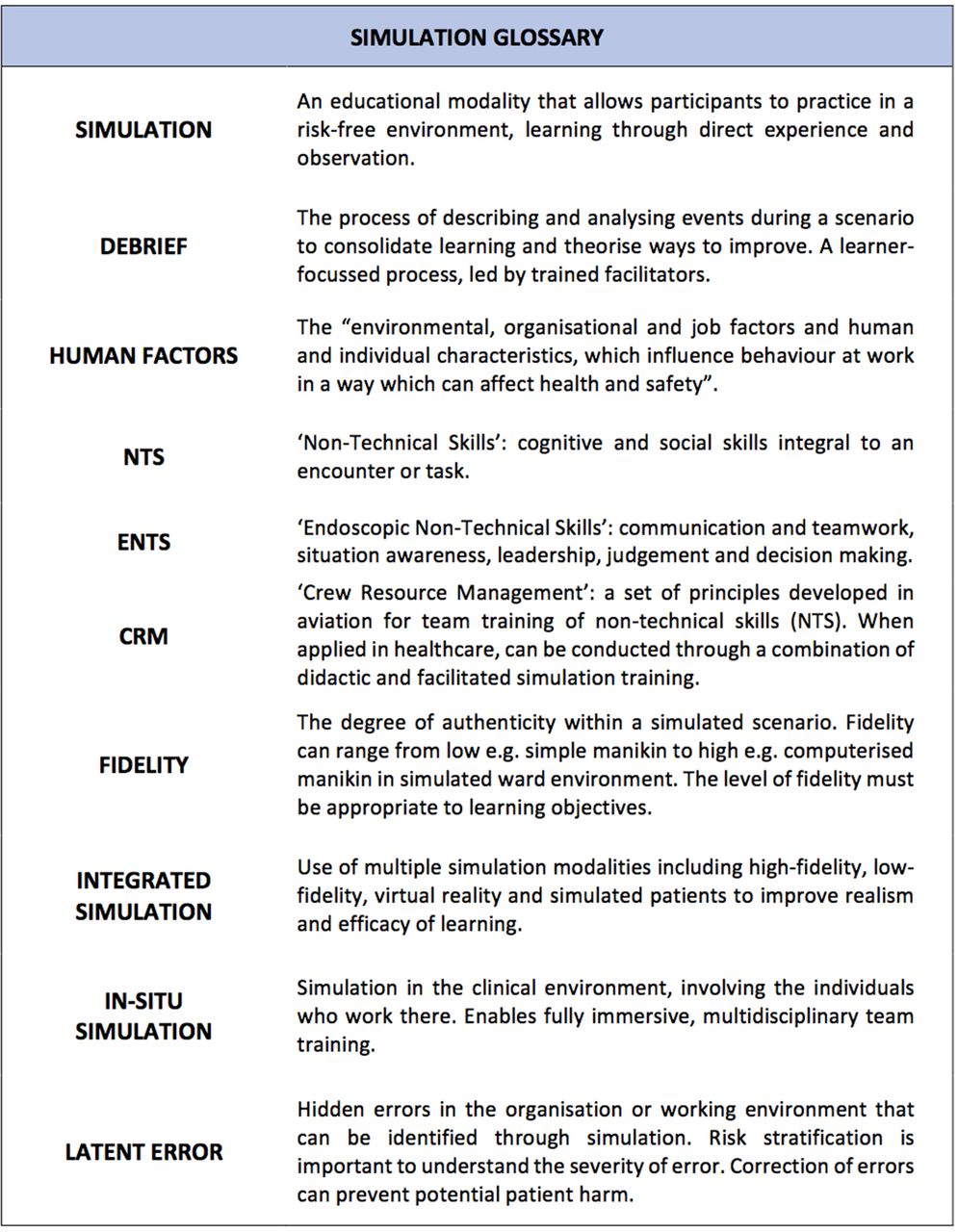
A glossary of terms relevant to simulation in endoscopy. CRM, Crew Resource Management; ENTS, Endoscopic Non-Technical Skills.
What are human factors?
‘Human factors refer to environmental, organisational and job factors and human and individual characteristics, which influence behaviour at work in a way which can affect health and safety’
(Health & Safety Executive,11)
Human factors encompass a wide range of elements contributing to safety, ranging from organisation and staffing to individual and team characteristics, which include NTS. Human factors research incorporates methods to develop NTS training and the design of systems and processes.12
What are ENTS?
NTS are cognitive and social skills that influence quality and safety outcomes.13 ENTS are classified into four domains: (1) Communication & teamwork, (2) Situation awareness, (3) Leadership and (4) Judgement & decision making. JAG recently introduced the ENTS framework into DOPS for diagnostic and therapeutic endoscopy in 2016 (table 1 14). The ENTS framework was developed from those used in anaesthetics and surgery, which have been used to drive assessment and subsequent quality assurance. Preliminary results suggest that ENTS correlate well with other assessable DOPS domains, demonstrating its construct validity.15
ENTS framework14
The ISREE strategy outlines the need for a focus on ENTS training. Strategies such as small group, didactic teaching,9 didactic training within a wider, structured endoscopy curriculum16 and e-learning (https://www.e-lfh.org.uk/programmes/endoscopy/) have been used in recent years but the optimal format of delivery remains unclear.
How can simulation reduce error and improve patient safety?
Simulation allows participants to practice within a controlled, risk-free environment, followed by a period of reflective analysis or ‘debrief’ in order to consolidate knowledge. There can be various levels of fidelity of the simulated environment targeted towards specific learning needs.
Simulation in NTS training has been used in various healthcare settings for some time, drawing on Crew Resource Management (CRM) principles in aviation. Within healthcare, it is known that poorly functioning teams can increase the risk of error and patient harm.17 CRM is designed to reduce error and improve safety through team training in NTS, developing and reinforcing ‘effective teamwork behaviours’.18 In healthcare, simulated team training can lead to increased confidence and better team working.19 It has been demonstrated to improve patient outcomes in critical care20 and reduce surgical mortality.21 Additionally, simulation may lead to improved patient outcomes over other forms of NTS training.22 Alongside individual studies, a systematic review of the healthcare literature identified that team processes significantly impact on clinical performance and that CRM training can reduce complication rates, morbidity and mortality.23 It has been suggested that systematic team training in NTS is integral in change to safer practice.24 25
Nationally, there appears to be a call for implementation of simulation-based education with both the Chief Medical Officer,26 and Department for Health recognising the potential benefits to patient safety.27
What about simulation in endoscopy?
Simulation is not new to endoscopy training. Over the past two decades, there has been widely documented use of simulation to develop technical proficiency through animal, mechanical and screen-based virtual reality (VR) simulators.28–30 The development of ENTS simulation training however, is relatively new. There have only been a handful of interventions developed, largely published in abstract format. In their review of the literature, Hitchins et al3 found only seven studies relating to NTS training in endoscopy, six of these used simulation. There have been no studies of endoscopy simulation looking directly at patient outcomes. In the following sections, the simulation modalities that have been used in ENTS training are described.
What is integrated simulation?
The concept of integrated simulation was pioneered by Kneebone and Darzi’s group in the early 2000s. The group studied nurse endoscopists ‘performing’ flexible sigmoidoscopy on simulated patients using VR simulators.31 Alongside demonstrating technical ability, participants had to interact and engage with their ‘patients’ in, as the authors described, a ‘quasi-clinical’ environment. Authenticating the task of endoscopy, through addition of an actor, added an additional level of realism with participants finding this ‘integration’ of technical and communication skills useful. Subsequently, several simulation programmes have developed ‘CRM-style’ scenarios using a combination of VR simulation, high-fidelity manikins and simulated patients to recreate emergency situations during endoscopy.32–34
El Menabawey et al32 recently described a 5-year experience of the ‘HiFIVE’ (Human Factors in Virtual Endoscopy) course. Designed around rare but serious incidents arising within endoscopy, it focuses on a wide range of human factors and has been recently refined to incorporate the different elements of the ENTS framework. A combination of VR simulation and simulated patients is used. Scenarios reflect emergencies in endoscopy or focus on specific skills away from the endoscopy theatre such as breaking bad news. Over 8 courses involving 44 participants (doctors, nurses and healthcare assistants), there was a significant improvement in participants’ confidence in several ENTS domains. Additionally, strategies for improving future practice and improved patient centeredness were identified as positive outcomes by learners. Several authors describe the use of integrated scenarios in response to clinical incidents or gaps in knowledge. Examples included management of respiratory complications following sedation33 and major haemorrhage during endoscopic haemostasis.34
One disadvantage of integrated simulation is the relative cost associated with its delivery. A combination of simulation equipment, actors, facilities and support staff is necessary for effective training. Funding streams may need to be sought, for example through educational grants. The notion that the beneficial impact of training may outweigh costs in the long term is attractive but difficult to demonstrate in real world analyses.35 Additionally, the need for trained faculty and a simulation environment are two factors that may prevent successful delivery of integrated simulation. As simulation becomes more prevalent, these may begin to be addressed.
What is in situ simulation?
In situ simulation involves the delivery of simulated scenarios in the clinical environment, involving participants undertaking normal duties.36 The concept is to promote fully immersive, multidisciplinary team training within the workplace making learning directly transferable to the real world. Scenarios can involve high or low fidelity manikins and mobile simulation equipment that can be setup within a bed space or clinical area.
In situ simulation has been shown to benefit team training, with perceived improvements in teamwork, and eventually patient outcome.37 It is an emerging simulation modality in endoscopy with an estimated prevalence of 2% worldwide.36 Where it is used, endoscopy staff find it to be a ‘useful’ and ‘realistic training experience’.38 Within the UK, only three sites have shared results of their endoscopy in situ programmes.39–41 These studies are summarised in table 2.
Endoscopy in situ simulation in the UK
In situ simulation can be versatile and reactive to the pressures of the working environment. Delivering sessions regularly allows training to quickly respond to clinical incidents. In addition, new guidelines or policies can be incorporated into the training to keep staff updated so important learning is disseminated. Minimal preparation is required, with lower costs compared with conventional simulation.42 As training is delivered directly in the working environment, staff do not require time away from their workplace or the need to rearrange commitments.
A significant challenge of in situ simulation is effective delivery, which may be challenging on a busy endoscopy unit. Solutions including careful planning and protected training are conceivable but feasibility of regular training may be impacted. Other drawbacks also include the use of medical equipment in training, infection control risks and intensity of labour for the team delivering simulation.43 Furthermore, the interruption of clinical duties may be perceived as a negative feature of in-situ simulation. There is some evidence to suggest that the introduction of training may overcome this short-term impact with long-term organisational gains.43 Similarly, patient advocacy groups acknowledge ‘brief delays in care’ as a result of in situ simulation being ‘outweighed by the value’ of team training.44
What are latent errors and why are they important?
A further benefit of practising in the low-risk, in situ environment is the detection of latent errors. These are failures in organisation or environment that can impact on patient safety. Discovery of errors can prompt interventions that ultimately improve patient safety, reflecting system ‘resilience’.12 Several examples have been documented within endoscopy, including the lack of Sengstaken-Blakemore tubes on the unit and malfunctioning emergency bells.40 41 This reflects a development in patient safety culture whereby training is reactive, responding to clinical incidents, and also proactive, preventing potential harm before it occurs.
Risk matrices can be used to quantify the impact of errors, and these are based on risk consequence and likelihood. ‘Consequence’ describes the effect on the patient and ‘likelihood’ outlines how common these events occur. These are combined to create a score. Within simulation training, latent error reporting includes the type of error (medication, equipment, environment, staffing or training) alongside risk assessment.45
Combining system evaluation and teamwork training synchronously is an effective improvement strategy for a healthcare organisation. However, it is imperative that robust reporting tools are in place so that identified latent errors are acted on and managed appropriately. Identified latent errors should be reported using local incident reporting tools. Representation of the simulation team on local patient safety committees allows clinical incidents to be assimilated into training scenarios, identified latent errors discussed and any necessary actions undertaken with efficiency and transparency.
Can I implement simulation in my department?
Implementation of simulation training requires input from multiple stakeholders. There are many factors to consider and the Association for Simulated Practice in Healthcare (ASPiH) provide a set of standards for introducing simulation at various levels.46
In situ simulation
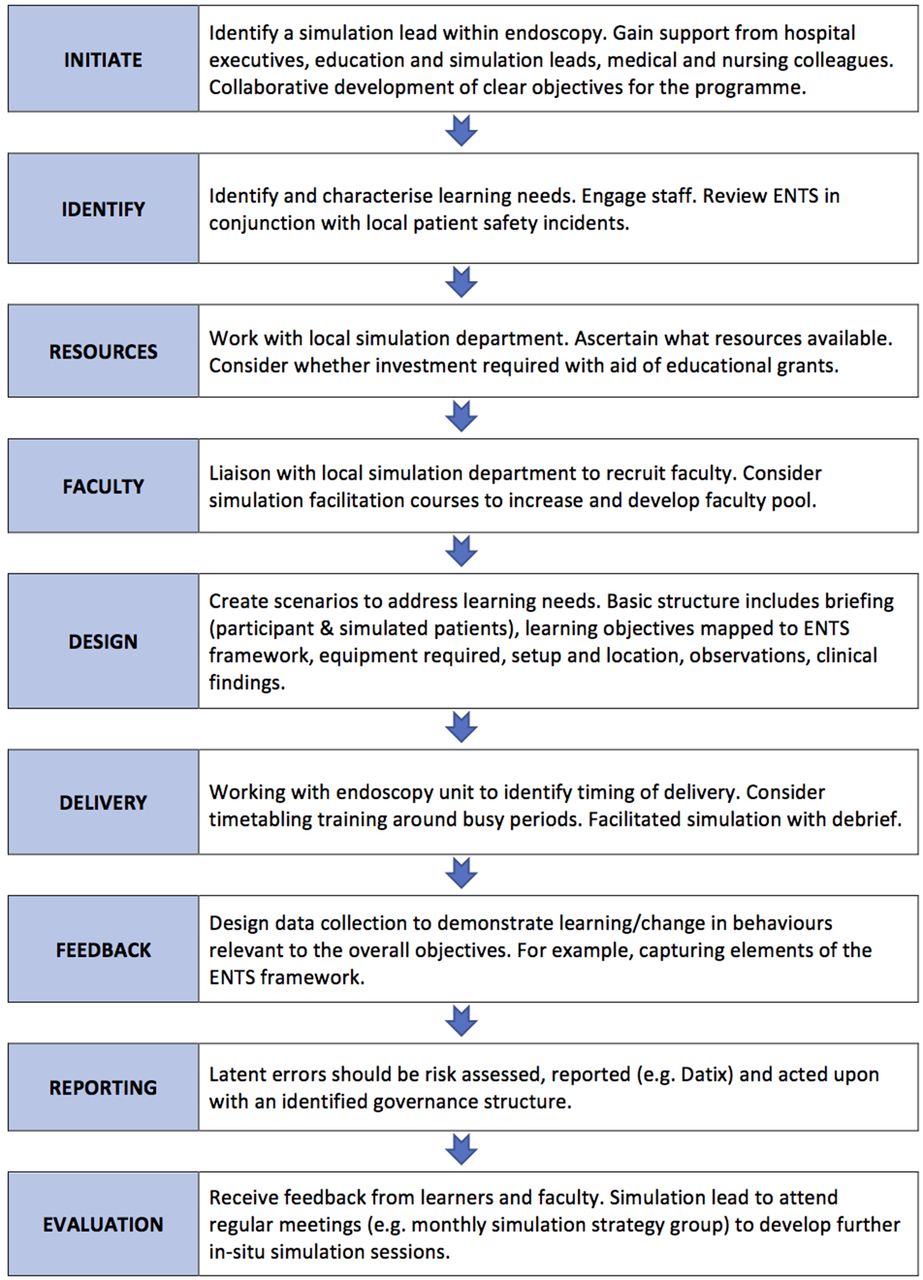
At the most basic level, low fidelity manikins and simple monitoring equipment are enough to create an in situ simulated scenario. However, there are numerous factors to consider before arranging sessions. As a summary, a basic ‘How to’ guide (see figure 2) describes the steps required to implement in situ simulation at a local level, based on the published guidance, ASPiH standards and the authors’ experiences.

How to implement in situ simulation in a local endoscopy unit.27 36 43 46 ENTS, Endoscopic Non-Technical Skills.
Integrated simulation
The development of integrated simulation training through local courses requires significant amounts of planning and a dedicated simulation department and faculty. These could be developed as part of a regional strategy, but require investment and ongoing evaluation to achieve sustainability.47 Part of the ISREE strategy is to understand how regional centres can provide ENTS training in this manner including centrally run courses or visiting faculty. The JAG QA-T group are in the process of developing pilot programmes in line with this approach.
What does the future hold?
A national simulation strategy incorporating the ENTS framework is the next step to improving training in human factors. Flin stated that NTS training is unlikely to change professional behaviours unless it is properly incorporated into educational and safety management systems.25 Integrated simulation courses and in situ simulation programmes could be developed for teams alongside existing training opportunities. This would vary across regions dependent on simulation availability. A standardised approach to team training has been shown to improve patient outcomes. Initiatives such as TeamSTEPPS,48 and the TRANSFORM Patient Safety Project,49 use a multilevel approach incorporating simulation. The high implementation costs of such strategies may be a limitation of their use in endoscopy; however, elements of these programmes may be replicable and a worthwhile consideration. On a smaller scale, one group has demonstrated that implementation of an NTS curriculum (didactic teaching combined with integrated simulation) was superior to simulation alone in a randomised trial.50 Thus, development of a novel curriculum may be one strategy worth pursuing.
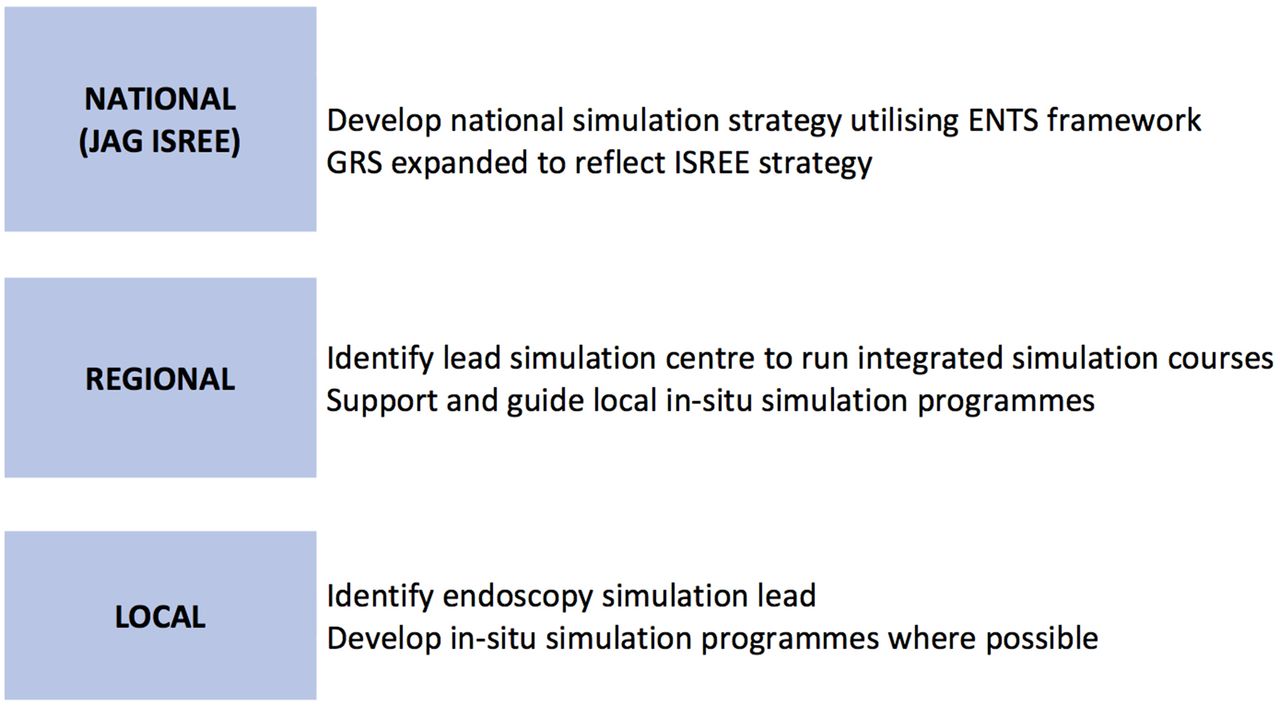
An example of how simulation implementation may look in the UK is proposed in figure 3.

{kind=link}
{kind=link}
{kind=link}
National, regional and local responsibilities for implementing ENTS simulation training. ENTS, Endoscopic Non-Technical Skills; ISREE, Improving Safetyand Reducing Error in Endoscopy.
Conclusion
There is amassing evidence to demonstrate the benefit of simulation training in developing NTS and improving patient outcomes across healthcare. Although the literature base is small, we have seen promising results in endoscopy through integrated and in situ simulation programmes which have a focus on human factors and ENTS. Added benefits such as latent error detection provide a further justification for their use.
Development of ENTS simulation training should be in line with the ISREE strategy, guided by the ASPiH standards. Individual departments should be encouraged to begin developing their own simulation practice, in situ being a good starting point. Nationally, there will need to be a focus on how simulation can be incorporated alongside existing training. A further focus of ISREE is to monitor outcomes, measuring the effectiveness of simulation thus improving the quality of evidence available. Future areas of investigation may also include exploring current use of simulation within UK endoscopy and accessibility of resources.
Evidently, there is much to consider in the coming years; however, it is clear that use of simulation training is another key step towards improving safety and reducing error in endoscopy.
Acknowledgments
None
References
Footnotes
Contributors SR drafted and edited the article. SM, ST-G and EW reviewed and edited the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ST-G is Chair of Joint Advisory Group for Gastrointestinal Endoscopy (JAG). She has received academic honoraria from Olympus, course fees from Aquilant/Fujifilm and equipment loans from Pentax and Olympus.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- UpFront