Article Text

Abstract
Objective To determine the challenges in diagnosis, monitoring, support provision in the management of inflammatory bowel disease (IBD) patients and explore the adaptations of IBD services.
Methods Internet-based survey by invitation of IBD services across the UK from 8 to 14 April 2020.
Results Respondents from 125 IBD services completed the survey. The number of whole-time equivalent gastroenterologists and IBD nurses providing elective outpatient care decreased significantly between baseline (median 4, IQR 4–7.5 and median 3, IQR 2–4) to the point of survey (median 2, IQR 1–4.8 and median 2, IQR 1–3) in the 6-week period following the onset of the COVID-19 pandemic (p<0.001 for both comparisons). Almost all (94%; 112/119) services reported an increase in IBD helpline activity. Face-to-face clinics were substituted for telephone consultation by 86% and video consultation by 11% of services. A variation in the provision of laboratory faecal calprotectin testing was noted with 27% of services reporting no access to faecal calprotectin, and a further 32% reduced access. There was also significant curtailment of IBD-specific endoscopy and elective surgery.
Conclusions IBD services in the UK have implemented several adaptive strategies in order to continue to provide safe and high-quality care for patients. National Health Service organisations will need to consider the impact of these changes in current service delivery models and staffing levels when planning exit strategies for post-pandemic IBD care. Careful planning to manage the increased workload and to maintain IBD services is essential to ensure patient safety.
- inflammatory bowel disease
- health service research
- infectious disease
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Summary box
What is already known on this topic
COVID-19 pandemic is expected to pose a myriad of challenges to National Health Services.
Essential services for inflammatory bowel disease (IBD) patients including outpatient care, advice lines, endoscopy and infusion units may be affected.
What this study adds
This survey evaluates the challenges to IBD services during the pandemic and the adaptations to meet these challenges.
There is significant reduction in staffing resources for the IBD team and significant increase in IBD advice line contact.
Face-to-face consultations in outpatients, non-emergency endoscopies and elective IBD have been significantly curtailed.
There is increased uptake of telemedicine, virtual multidisciplinary team meetings and non-invasive monitoring of patients.
Summary box
How might it impact on clinical practice in the foreseeable future
There is urgent need to review models of care and staffing levels of IBD service in planning exit strategies in the post -pandemic period.
Insights gained from the rapid adaptations by services during the peak of the pandemic may present opportunities for positive changes in IBD services.
Introduction
The COVID-19 pandemic has significant implications for the diagnosis and management of patients with gastrointestinal conditions including inflammatory bowel disease (IBD).1 Healthcare systems have had to adapt rapidly to maintain provision of core services and reduce unintended consequences from the necessary diversion of resources to focus on the pandemic. The continued accumulation of cases positive for SARS-CoV-2 and the intervention from national governments to enforce strict social isolation (‘shielding’) and distancing have necessitated IBD services to dramatically changing and restructuring the way they provide care for IBD patients.2 In addition, the rapid increase in COVID-19 hospitalisations along with restrictions in endoscopic and surgical facilities has resulted in the redeployment of clinicians and nurses to front-line services to care for these patients with resultant impact on the delivery of IBD care.3 In IBD, delays in diagnosis and therapy can have serious consequences including the need for emergency surgery.4
Patients are understandably concerned about the impact of their IBD and its treatment on their risk of severe COVID-19 disease. However, it is important that IBD patients continue to attend for inpatient, day case and outpatient hospital care for the management of active disease and complications and for therapies such as intravenous biologics. Furthermore, given that immunosuppressive and biologic agents form the cornerstone of IBD management, concerns have been raised that patients with IBD may be more susceptible to SARS-CoV-2 infection and whether they may have poorer outcomes if infected with the virus.5 6 Although there are, as yet, no specific data quantifying additional risk, specialist societies and expert groups have recommended heightened vigilance.7–9 In the UK, patients categorised as high risk have been recommended for isolation (‘shielding’) by UK Department of Health and Social Care,10 requiring individual IBD services to rapidly identify individuals in this group using hospital databases and registries.
The UK has a strong record of providing personalised multidisciplinary care for patients with IBD. Successive IBD audits have shown improvements in resource provision (including IBD nurses) and overall quality of care.11 12 More recently, a multidisciplinary stakeholder group has proposed key quality standards for IBD care in the UK.13 Maintaining high-quality care during the COVID-19 pandemic will remain a constantly evolving challenge. IBD clinicians and specialist nurses across the UK have formed an IBD COVID-19 working group to share expertise and promote a collaborative and co-ordinated nationwide approach to meet the challenges posed by the pandemic. This has enabled the development of a UK consensus on management of IBD during the COVID-19 pandemic.8
The impact of the COVID-19 pandemic on provision of IBD care has not been previously evaluated. Most centres have rapidly and independently reconfigured their services guided by local management decisions based on varying service needs, redeployment of some of their staff and reconfiguration of available healthcare facilities. There has been limited opportunity or time to share experience of service reconfiguration to determine the impact across regions. We surveyed adult and paediatric gastroenterology services caring for IBD patients in the UK to assess the impact of COVID-19 on service delivery.
Methods
We developed an internet-based survey using Google Forms (Google, California, USA) to assess changes to IBD service provision in the COVID-19 period. This was circulated to IBD services throughout the UK through the membership of the UK IBD COVID-19 working group and social media. The Royal College of Nursing (RCN) IBD specialist nurse network and the service leads of the services participating in the IBDUK self-assessment were also invited to participate. Furthermore, the survey was emailed to the membership of the British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN). Survey participation was voluntary, and the option was given to provide the National Health Service (NHS) Trust identity and contact details with the option of being contacted for future surveys related to this subject. The survey was carried out between 8 and 14 April 2020, which corresponded to 1 month after the UK government decision for lockdown. The survey (included in online supplementary appendix) covered the characteristics and staffing resources of the services, the changes instituted in provision of IBD care in preparation for the COVID-19 pandemic and the impact of the pandemic on the provision of IBD services. Data were collected in Google Docs and then exported for analysis to Microsoft Excel (Microsoft, Washington, USA) and R V.3.6.0 (R Foundation for Statistical Computing, Vienna, Austria). Where more than one response was received from the same IBD service, the most recent response was used, though paediatric and adult services were counted as separate. Response frequencies were tabulated and expressed as percentages of total responses; where there were incomplete responses to a question, this is reflected in the relevant denominator. Wilcoxon signed-rank tests were used to compare paired continuous variables. Fisher’s exact test was used to compare categorical data.
Supplemental material
Results
Respondents
We received 147 responses representing 125 IBD services (England 106, Scotland 9, Wales 8 and Northern Ireland 2) representing approximately 70% of the IBD services in the UK (paediatric services 19% of the total). Respondents included 65 (44%) adult gastroenterologists, 53 (36%) adult IBD nurses, 21 (14%) paediatric gastroenterologists, 6 (4%) paediatric IBD nurses and 1 IBD surgeon. Only the most recent response for each service was used. Fifty-seven per cent (71/124) were dedicated IBD services and 43% (53/124) were general gastroenterology services providing IBD care. Fifty-seven per cent (70/123) of the services were based in a university teaching hospital, while 42% (52/123) were based in district general hospitals. All services who responded were based in public hospitals in the UK NHS.
Impact on work force
The overall number of whole-time equivalent (WTE) gastroenterologists and IBD nurses providing elective outpatient care decreased significantly between baseline (median 4, IQR 4–7.5 and median 3, IQR 2–4) to the point of survey (median 2, IQR 1–4.8 and median 2, IQR 1–2) 6 weeks following the onset of the COVID-19 pandemic (p<0.001 for both comparisons). The proportion of services with more than three WTE gastroenterologists providing IBD care was 81% (100/124) at baseline but fell to 34% (41/122) as a result of reconfiguration (p<0.001), with 8% (10/122) services having no dedicated IBD clinician in the COVID-19 era. Similarly, the number of services with more than one WTE IBD nurse fell from 81% (100/124) to 53% (63/118) (p<0.001). Eight per cent (9/118) of services stated that they had no provision for IBD nurse care. The main reasons given for the reduction in gastroenterologists and IBD nurses were redeployment (51% (64/125) and 40% (50/125), respectively), self-isolation due to COVID-19 symptoms (22% (27/125) and 17% (21/125)) and belonging to the shielding category (9% (11/125) and 14% (18/125)). The number of WTE nurses in adult IBD services dropped significantly from median 3 (IQR 2–4) to 2 (IQR 1–3, p-value<0.001). In paediatric services, the median number of nurses was 2 (IQR 1–2) prior to COVID-19 and 1 (IQR 1–2) in the COVID-19 era (p=0.24).
The median number of WTE gastroenterologists and IBD nurses required to provide IBD care for adult patients as self-assessed by our respondents were 4.0 (IQR 2.4–5.0) and 3.0 (2.0–4.0), respectively. For paediatric services, the median number of WTE gastroenterologists and IBD nurses required to provide IBD care was reported as 2.0 (IQR 1.0–3.0) and 1.0 (1.0–2.0), respectively. When asked about the possibility of reduction in staff numbers below this required number as a result of COVID-19, 60% (72/119) of services thought this was certain or highly likely for gastroenterologists and 63% (70/123) for IBD nurses (figure 1).

Likelihood of having less than the minimum number of required IBD healthcare professionals during the COVID-19 era. IBD, inflammatory bowel disease.
Only 7% (9/125) of services reported that their IBD nurses could maintain their normal service. IBD specialist nursing support for inpatients was either not available for 26% (32/125) or curtailed by 31% (39/125) of the services. Similarly, nurse-led outpatient clinics had been suspended by 27% (34/125) and reduced in a further 26% (33/125) of services.
Impact on IBD service functions
Clinics
Significant changes were reported in the provision of outpatient IBD clinics. No service reported continuing normal activity with routine face-to-face appointments. Nine per cent of services reported running face-to-face clinics with reduced capacity, and 30% (38/125) reported complete cancellation of routine clinics. Face-to-face clinics were substituted with telephone consultation by 86% (108/125) and video consultation by 11% (14/125) of services; most services (13/14) using video were also using telephone consultations. The proportion of patients reviewed using telephone clinics was 100% in half of services (61/124) and above 50% in a further 32% (40/124). In contrast, only 19% of services (23/123) reported having access to video consultation, with the majority (20/25) having access to video facilities reporting that they used them for less than a fifth of their consultations. We observed the use of patient apps in some services with 6% (7/123) and 14% (17/123) of respondents, respectively, reporting current use or in set up.
Infusion services
Drug infusion services were relocated to a ‘safer area’ away from acute services by 50% (62/125). The majority, 62% (77/125), reported performing a prescreening check list for COVID-19 before patients were invited to attend infusion services for treatment. Most services (77%, 96/125) reported maintaining infusion intervals with ‘enhanced provisions’ to reduce transmission but 11% (14/125) reported delaying treatment. Masks were reported as being used by staff in 61% (76/125) of services and by patients in 24% (30/125). Seven per cent (9/125) of services reported proactively switching their patients from intravenous to subcutaneous biologics. Sixty-two per cent (78/125) of services reported patient-initiated cancellation of at least some infusions; the most frequently reported proportion was approximately 10% of patients. Patient-reported reasons for cancellation included self-isolation due to COVID-19 symptoms and fears and concerns about therapies. Iron infusion services have been completely stopped by 16% (20/125) or curtailed by 45% (56/125) of services, respectively.
IBD advice line
The majority of services (94%; 112/119) report an increase in IBD advice line activity, with 80% (95/119) reporting a more than 50% increase and 34% (41/119) reporting a more than doubling of activity (figure 2).

Change in inflammatory bowel disease advice line calls during the COVID-19 era.
Services are adapting to this increased demand using strategies such as an automated email (41%; 51/125), voice message response (45%; 56/125), more contact options (12%; 15/125) and additional staff overseeing/providing IBD advice line services (10%; 13/125). Conversely, 29% (36/125) have reported a reduction in the number of staff providing advice line services.
Homecare services
Twenty-seven per cent (33/121) of services reported an inability to set up new homecare services for subcutaneous biologics and immune-modulatory therapy. In addition, 20% (25/122) also experienced disruption to the homecare delivery provision of therapies due to provider issues (28%; 3/125), blood monitoring issues (5%; 6/125), pharmacy issues (4%; 5/125) and a reduced number of nurses (5%; 6/125).
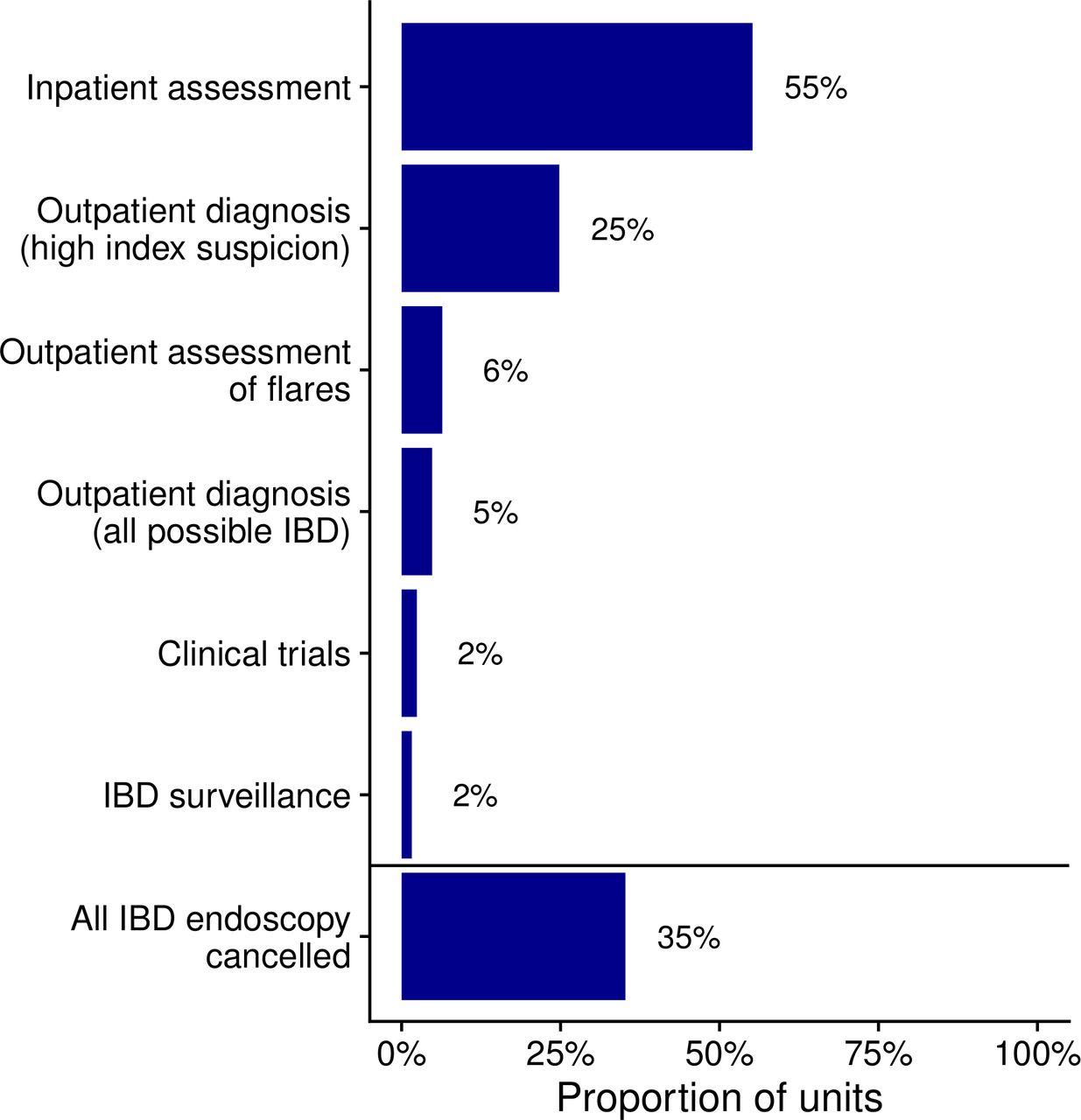
Endoscopy
In keeping with national guidance,14 endoscopy activity has been significantly curtailed for IBD patients with current provision only being available for defined high priority indications (figure 3). In 35% (44/125) of services, all IBD-related endoscopy activities have been cancelled.

Endoscopy provision during the COVID-19 pandemic. IBD, inflammatory bowel disease.
Provision of IBD surgery
Potential elective surgery for IBD has been put on hold/withheld in all services surveyed. Indications for surgery that may be permitted include emergency small bowel resections in 74% of services (93/125), colectomy for acute severe colitis in 72% (90/125), perianal surgery in 42% (52/125) and colectomy for IBD dysplasia in 4% (5/125). In 10% (13/125) of services, all IBD surgery has been stopped.
IBD multidisciplinary team meetings (MDTs)
All IBD MDTs have been cancelled in 28% (34/122) of the services, while 40% (49/122) have converted them to virtual MDTs. Twenty-five per cent (30/122) of services are still running face-to-face MDTs, but with reduced capacity and/or social distancing. A small proportion either have put in place alternative arrangements (2%; 3/122) or never had MDTs to start with (5%; 6/122).
Laboratory services
Less frequent blood monitoring regimens for patients on immunomodulators have been adopted by 65% (79/121) of services, while 6% (7/121) have stopped all routine blood monitoring. The remainder of services (29%; 35/12) reported that they were continuing normal monitoring arrangements.
There was significant variation in the provision of laboratory faecal calprotectin testing. A quarter of services (33/122) have no access to faecal calprotectin, while a further 32% (39/122) have reduced access. Point-of-care calprotectin has been introduced in 5% (6/120) of services and scaled up in 2% (3/120); however, most services do not have access to point-of-care calprotectin analysis.
Flare services
Only half of the services (50%; 63/125) are providing access to face-to-face flare clinics. However, 77% (96/125) have access to blood tests in secondary care and 62% (77/125) to blood tests in primary care, while 12% (15/125) of services report no access at all to blood tests for flare. Fifty-eight per cent (73/125) had access to faecal calprotectin testing (home or laboratory for flare managements). Endoscopy was only being used to assess suspected flares in outpatients with known IBD in 6% (8/125) of services.
Identification of high-risk patients
The UK Government introduced guidance on 21/22 March 2020 to protect patients at risk of contracting COVID-19 based on emerging world data/medical advice. The concept of shielding was introduced, requesting patients in the highest risk category to withdraw from society in their own homes for a period of 12 weeks. To support this endeavour, specialist societies including the British Society of Gastroenterology developed guidance to risk stratify patients.8 NHS trusts and health boards then had to identify the highest risk patients based on these criteria. At the time of the survey, 61% (76/125) of services reported having undertaken identification of high-risk patients who meet the criteria for shielding in their IBD cohorts and 76% (95/125) have already communicated with their highest risk patients. Furthermore, 34% (42/125) of the services have communicated with their moderate risk patients. Seventy eight per cent of services (96/123) reported an intention to participate in the SECURE-IBD registry (https://covidibd.org), which is recording the number of COVID cases in IBD patients; this includes 11% (14/123) who had already entered patients.
Geographic variation
Exploration of the variation in provision of services around the UK, including faecal calprotectin, endoscopy and surgery, did not reveal any particular clustering of loss of service into one region of the country (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Geographic variation around the UK in changes to provision of (A) faecal calprotectin, (B) endoscopy and (C) surgery. IBD, inflammatory bowel disease.
Discussion
The COVID-19 pandemic is having a pronounced impact on the lives of patients and healthcare professionals (HCPs). IBD services in the UK meanwhile have also needed to adapt their priorities rapidly and modify current models of service to ensure delivery of a minimum standard of safe and effective care. This involved an urgent redesign of clinical services with clear communication among HCPs to develop an iterative model of care, responsive to the challenges posed by the unpredictable pandemic. The aim of this survey from the UK IBD COVID-19 working group was to explore, consider and disseminate examples of dynamic models of service provision.
Dramatic and significant reductions in staffing levels have inevitably impacted negatively on service provision and delivery. This has affected routine care for people with IBD including disease and treatment monitoring, clinical and endoscopic assessment, endoscopic surveillance, access to elective and semiurgent surgery and multidisciplinary team working. Despite this, most services have been able to adapt and have been innovative with service delivery and models of care with the aim of providing safe and effective care.
The unprecedented scale of this pandemic and uncertainties driven by the absence of ‘effective’ treatment for COVID-9 has important implications for contingency planning with existing, evolving and aspirational models of care delivery. Important elements such as staffing levels from redeployment, provision of ‘adequate’ monitoring, clear routes of access to specialist advice and urgent review, and the ability to start, continue and monitor effective therapies and outcomes will need careful consideration.
The high level of contact with IBD services by patients since the start of the pandemic demonstrates the ongoing requirement for suitably staffed advice lines and access to expert review, whether by telephone, video or face-to-face clinics.
Wherever possible, arrangements should be made to facilitate some method of ongoing regular, scheduled MDT working, for discussion of complex or concerning cases needing consensus opinion. In addition, there will arguably be benefit to all team members of accessing peer and colleague support. Videoconferencing platforms provide a means to facilitate such discussions while ensuring staff can practise social distancing and, where possible and appropriate, work remotely. Where scheduled MDTs, either virtual or face to face, are no longer feasible due to changes in work schedules, other models of delivering care could be considered. Informal arrangements such as discussion by email involving a suitable mix of specialist can provide short-term alternatives.
There has been rapid uptake by services of telephone clinics, and some centres have instituted video consultations. Previous studies15–17 have assessed the impact of telemedicine systems in IBD assessing feasibility, patient acceptance, effectiveness and impact on healthcare utilisation. However, there are several potential barriers18 and further adoption and upscaling of teleconsultation tools are urgently warranted. There is an ongoing international survey of telemedicine in IBD in the COVID-19 era organised by the International Organisation for the Study of IBD.
IBD patients appear to be receptive to the idea of non-face-to-face review where appropriate, with low levels of non-attendance reported to telephone and virtual appointments.19 Reviewing patients also provides an opportunity to check their understanding of the ongoing pandemic, the impact it has on them as individuals and any effect it may have on their treatment. This should promote adherence to therapy, as well as facilitating early management of disease flares. Future surveys should assess patients’ preferences for telemedicine as we plan services following the COVID-19 pandemic.
IBD endoscopy practice during the ongoing COVID-19 pandemic appears to be broadly in line with national and international consensus.14 20–22 Endoscopy services have been rationalised to provide the most urgent information for the safe care of patients such as in the management of acute severe colitis. Similarly, elective surgery has been stopped with a focus on emergency surgery for acute severe colitis, emergency small bowel resection and drainage for perianal sepsis. There are concerns about the potential impact of delaying elective endoscopies and operations in patients with IBD. Services will need to make plans for appropriate prioritisation of delayed procedures including those needing diagnosis of new IBD or/and those needing surveillance to ensure safety in the post-pandemic era.22
Currently, the UK consensus guidelines do not recommend cessation of therapies such as biologics and immunomodulators in IBD patients who currently do not have COVID-19.8 In those who stop therapies during illness with SARS-CoV2 or following a positive test, current guidelines recommend that biologics and immunomodulators are recommenced soon after cessation of symptoms.8 9 The IBD services surveyed here appear to have taken prompt action to ensure continuity of treatments in infusion units, but logistical challenges with location and delivery of treatments remain; a significant proportion of services reported difficulties in delivery of infusions. This may worsen as the pandemic progresses over time due to patient factors such as shielding, isolation due to contact and fears about safety as well as staffing-related challenges depending on the duration of the pandemic or indeed new peaks in the pandemic. Adoption of subcutaneous therapies among patients starting biologic therapy may reduce the pressures on infusion units and reduce patient footfall in the hospital site. However, a concerning number are reporting difficulties in starting new home care treatments and also in the delivery of ongoing treatments, which needs addressing urgently.
IBD advice lines are an immensely valuable resource for patients with IBD,23 and this is more so when elective activity has been curtailed as evidenced in our survey. The marked increase in the number of patients accessing IBD advice lines, coupled with a reduction in the number of staff in more than a quarter of services, is likely to impact provision of prompt support and advice to patients, who are understandably concerned about the potential impact of IBD and their medications during the COVID-19 pandemic. Services have attempted to provide more online support, but the unprecedented increase in number of contacts may prove overwhelming. It is likely that requests for advice regarding social distancing and shielding will reduce, but the number of patients contacting IBD advice lines for flare management may rise as routine outpatient clinics have been stopped or have limited access in many centres.
Non-invasive assessment and monitoring of IBD are critical during the COVID-19 pandemic. Hence, it is unfortunate that several services report cessation of faecal calprotectin services, mainly due to concerns regarding risks to laboratory staff, although faeco-oral transmission is not confirmed yet. SARS-CoV-224 has been detected in faeces even in asymptomatic patients with COVID-19; however, it is not clear if this represents live virus. One option for such services is to initiate and upscale the use of point-of-care faecal calprotectin testing.25 A major concern highlighted by this survey is the significant reduction in both clinicians and specialist nurses available to care for IBD patients. More than 50% of the respondents felt that the services would remain understaffed and unable to meet the needs of IBD patients. Redeployment to front-line COVID-19 duties appears to be the main factor, and this may need addressing at unit level with measures such as creation of a designated core team of clinicians and specialist nurses to deliver IBD care, as adopted by centres in Italy.26 We should also ensure that, where the local COVID-19 situation permits, IBD specialist nurses and doctors are able to resume their responsibilities in IBD care.
Our survey has some limitations. We could not capture responses of all IBD services in the UK. We were, however, able to reach out to approximately 70% of UK IBD services who registered for the recent unit and patient assessment of services under IBDUK (https://ibduk.org/services-map). The epidemic is at different stages across the UK, but as can be seen in figure 4, we have good geographic coverage of the country. It is possible that some of the most under-resourced IBD services may also have been less likely to have someone available to complete the survey. Finally, the rapidly evolving nature of data and guidelines relating to COVID-19 in IBD make future assessment of service provision important to ensure equitable access to high-quality IBD care across the country.
Conclusions
In this survey, we provide a comparative reference to support consistency of care across the UK during a difficult time and to offer a template to centres in other countries, which have yet to undergo such alterations. It is our hope that this will allow services to make suitable arrangements to maintain high-quality uninterrupted care for patients with IBD. The ongoing COVID-19 pandemic has and may continue to pose myriad challenges to healthcare systems across the globe. IBD services in the UK and other countries will face unique challenges both during the peak and post-peak pandemic period with respect to responsive and responsible adaptation of service delivery. These are unprecedented and challenging times. Yet, even grim challenges present opportunities not in the least with insights gleaned from rapid adaptation of models of service delivery some of which are likely to be also suitable in a post-COVID-19 world. Indeed, there may be opportunities for positive changes in IBD services resulting from this difficult time.
Acknowledgments
The authors acknowledge Sue Protheroe and Carla Lloyd for sending e-mails to BSPGHAN members.
References
Footnotes
Twitter @DrNickKennedy, @PaedsRH, @ShahidaDin1, @DrPhilipJSmith
CWL and SS contributed equally.
Correction notice This article has been corrected since it published Online First. The author's name R Mark Beattie has been corrected and ORCID ID has been added and the acknowledgement statement has been updated.
Collaborators On behalf of the UK IBD COVID-19 working group (see appendix for details).
Contributors The original project was conceived by SS and the survey developed by SS, CWL, NAK, RH and LY. Analyses were performed by RH and NAK. The initial draft of the manuscript was written by SS, RH, LY and NAK. All of the remaining authors contributed to data collection and to further writing of the manuscript. The other listed contributors performed data collection. All authors and contributors were given the opportunity to review the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Deidentified participant data are available by request from the corresponding author.
Linked Articles
- UpFront