Article Text

Abstract
Objective The COVID-19 pandemic has placed increased strain on healthcare systems worldwide with enormous reorganisation undertaken to support ‘COVID-centric’ services. Non-COVID-19 admissions reduced secondary to public health measures to halt viral transmission. We aimed to understand the impact of the response to COVID-19 on the outcomes of upper gastrointestinal (UGI) bleeds.
Design/methods A retrospective observational multicentre study comparing outcomes following endoscopy for UGI bleeds from 24 March 2020 to 20 April 2020 to the corresponding dates in 2019. The primary outcome was in-hospital survival at 30 days with secondary outcomes of major rebleeding within 30 days postprocedure and intervention at the time of endoscopy.
Results 224 endoscopies for 203 patients with UGI bleeds were included within this study. 19 patients were diagnosed with COVID-19. There was a 44.4% reduction in the number of procedures performed between 2019 and 2020. Endoscopies performed for UGI bleeds in the COVID-19 era were associated with an adjusted reduced 30-day survival (OR 0.25, 95% CI 0.08–0.67). There was no increased risk of major rebleeding or interventions during this era. Patients with COVID-19 did not have reduced survival or increased complication rates.
Conclusion Endoscopy for UGI bleeds in the COVID-19 era is associated with reduced survival. No clear cause has been identified but we suspect that this is a secondary effect of the response to the COVID-19 pandemic. Urgent work is required to encourage the public to seek medical help if required and to optimise patient pathways to ensure that the best possible care is provided.
- gastrointestinal bleeding
- endoscopy
- therapeutic endoscopy
- oesophageal varices
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. De-identified participant data is stored on an encrypted password-protected computer in the Institute of Liver Studies, King’s College Hospital. Data is available on request from Dr OD Tavabie at oliver.tavabie@nhs.net.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Summary box
What is already known on this topic
The mortality and morbidity secondary to SARS-CoV-2 infection are increasingly well understood. Outcomes for other disease processes during the global pandemic are, however, less well defined.
What this study adds
Patients who underwent endoscopy in the COVID-19 era had reduced 30-day survival, but COVID-19 did not influence this outcome. There were no differences in rates of major rebleeding or therapeutic interventions, suggesting that this represents a secondary effect of the response to the COVID-19 pandemic.
How might it impact on clinical practice in the foreseeable future?
These data indicate the need for further public education to recognise medical emergencies and the requirement to seek urgent help appropriately. Patient pathways require critical review and optimisation to ensure that healthcare workers can provide the best possible patient care during the ongoing pandemic.
Introduction
The significant morbidity and mortality directly associated with SARS-CoV-2 infection necessitated substantial changes in healthcare provision with the closure of ‘non-urgent’ services and redeployment of specialty staff to the ‘frontlines’ of acute medicine. This ‘COVID-centric’ model has led to concerns about a potential reduction in the standard of care of patients with the non-COVID-19 disease. Medical societies have issued guidance regarding which services should continue and which could be suspended.1 2 Although this has been necessary to ensure an adequate response to the pandemic, there is concern that patients are fearful of attending hospital with life-threatening non-COVID-19 pathology. Following the UK lockdown on the 23 March 2020, a significant reduction in accident and emergency attendances was observed across all non-respiratory conditions.3 The impact of our response to this global pandemic on non-COVID-19 morbidity and mortality needs to be established.
Endoscopy services have adapted to the risk of SARS-CoV-2 transmission. Data suggest that the use of personal protective equipment (PPE) limits transmission particularly in aerosolising upper gastrointestinal (UGI) endoscopy,4 although recommendations differ between countries.1 4 5 Given these challenges, it is important to consider the risks and benefits of a procedure for both patients and staff. The British Society of Gastroenterology (BSG) issued guidance to support endoscopy units detailing emergency/essential endoscopic procedures that should continue, including management of UGI bleeding.1 However, there have been international reports of a significant reduction in the number of endoscopies performed for UGI bleeds since the beginning of the pandemic. It is unclear whether this is due to a reduction in patients presenting to the hospital or a higher threshold for endoscopy.6 7
We designed a multicentre retrospective cohort study to evaluate the impact of COVID-19 on the endoscopic management of UGI bleeds across London. We aimed to determine whether changes made in response to the pandemic affected the number of procedures performed, patient outcomes postendoscopy and the impact of SARS-CoV-2 infection on patient outcomes.
Materials and methods
Data collection
We conducted a multicentre retrospective cohort study across nine London teaching hospital sites. We identified all inpatient endoscopic procedures for UGI bleeds in adults performed from 24 March 2019 to 20 April 2019 (era 1) and 24 March 2020 to 20 April 2020 (era 2). One centre instead provided data from 1 April 2019 to 28 April 2019 for era 1 due to a lack of access to data prior to this period. Era 2 was selected as it began 7 days following the issuance of BSG endoscopy guidance,1 it included the first week of the UK lockdown, and the peak for London hospital admissions secondary to COVID-19 (figure 1A). The decision to perform a UGI endoscopy for a bleed was based on individual clinician judgement, rather than unit-wide operational policies. All sites have 24-hour on-call consultant-supervised UGI bleed cover and are situated within London boroughs with the highest mortality rates per population density from COVID-19 in the UK (figure 1B). Exclusion criteria included outpatient endoscopy for UGI bleeding and investigation for anaemia without evidence of acute GI blood loss. We interrogated electronic patient records. This study was registered as an audit at each participating site.
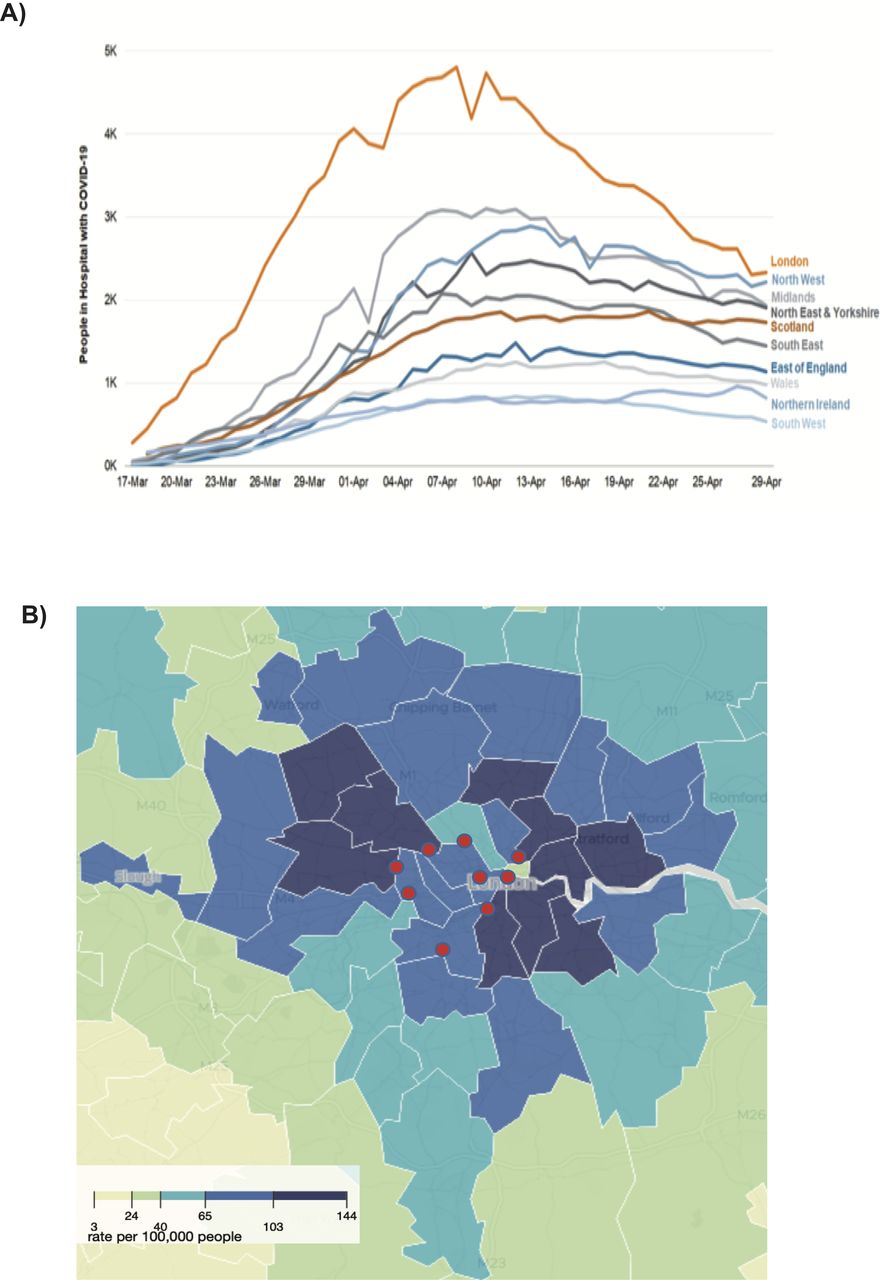
Indication of COVID-19 burden in London. (A) COVID-19 inpatient bed occupancy through March and April across the UK. Source: NHSE, Welsh Gov., Scottish Gov., Northern Ireland Executive licensed under the Open Government License v 3.0. Contains OS data Crown copyright and database right (2020).26 (B) Location of participating sites with mortality rate per population density secondary to COVID-19 plotted by local authority. Modified from source: Office for National Statistics licensed under the Open Government License v 3.0. Contains OS data Crown copyright and database right (2020).27
Variables
We developed a standardised proforma to record anonymised data, including age, sex, reason for admission (UGI bleed/other), time from referral to endoscopy (<24/>24 hours), presence of a consultant, timing of endoscopy (in hours (09.00–17.00)/out of hours (17.00–09.00)), location of endoscopy (critical care/theatres/endoscopy unit), admission Glasgow Blatchford Score (GBS), aetiology, therapeutic intervention (intervention/no intervention), haemostasis (achieved/not achieved), hospital length of stay and postendoscopy Rockall Score. For non-survivors, death certificates were examined for reference to GI bleeding. Patients were defined as having COVID-19 if they had a positive SARS-CoV-2 PCR result.
Outcome measures
The primary outcome was 30-day in-hospital survival with secondary outcomes being 30-day major rebleed incidence and endoscopic intervention. Individuals discharged before 30 days postendoscopy were assumed to have survived. Major rebleeding was defined as any patient requiring further endoscopy or radiological intervention within 30 days of endoscopy.
Statistical analysis
Comparisons were made between 2019 and 2020 cohorts and patients with and without COVID-19 in the 2020 cohort. Continuous variables were analysed for normality using the D’Agostino and Pearson tests. Normally distributed data were analysed using unpaired t-tests with results reported as mean (SD). Non-normally distributed data were analysed using the Mann-Whitney U test with results reported as median (IQR). Categorical variables were analysed by the Fisher exact test with results reported as number (percentage). Multiple logistic regression was performed to ascertain if UGI bleed endoscopy performed in 2020 and COVID-19 influenced the primary and secondary outcomes. We used complete case analysis, excluding individuals with missing data. Variables with a p value of <0.2 or of particular interest were included in each model and backwards elimination was performed. An R2 threshold with other variables within the model was set at <0.25 to reduce colinearity. Results were recorded as ORs with 95% CIs and p values. Correction for multiple comparisons was performed using the Benjamini-Hochberg procedure with a false discovery rate set at 0.05. Statistics were performed using Prism V.8.4.2 (GraphPad).
Results
Characterisation of patient populations
A total of 224 endoscopic procedures for 203 patients were included. There was a 44.4% reduction in the number of endoscopies with a significant reduction in 30-day survival in 2020 compared with 2019 (76.3% vs 91.7%) (table 1). Of the 31 non-survivors, only 3 had GI bleed recorded on their death certificates (all from era 1). Non-variceal endoscopy findings are recorded in the online supplemental table 1A,B.
Supplemental material
Baseline characteristics and clinical course of 2020 and 2019 cohort
Hospitals implemented SARS-CoV-2 screening policies at different time points. As such, 7 (9%) patients in the 2020 era were not screened. Within the 2020 cohort (table 2), 19 endoscopies were performed for patients with COVID-19. On univariate analysis, no significant differences were observed between those with COVID-19 and those without for 30-day survival or major rebleeding. Endoscopy was more likely to be performed on critical care for patients with COVID-19 (42.1% vs 16.4%); however, this was not significant following correction for false discovery. Patients without COVID-19 were more likely to be admitted due to a UGI bleed than those with COVID-19 (63.9% vs 21.1%).
Characterisation of endoscopies performed for patients with and without COVID-19
UGI bleed endoscopy in 2020 was an independent risk factor for reduced 30-day patient survival regardless of COVID-19 status
Across both cohorts, there were 193 endoscopies performed where patients reached 30-day survival and 31 where patients did not (online supplemental table 2). By univariate analysis, patients surviving at 30 days were more likely to have been admitted with a UGI bleed (62.7% vs 19.4%) and haemostasis achieved at the time of their initial endoscopy (92.7% vs 71.0%). Non-survivors were more likely to have had their endoscopy performed on critical care units (54.8% vs 8.3%), have higher GBS (12.0 vs 9.3) and Rockall Scores (6.0 vs 5.0).
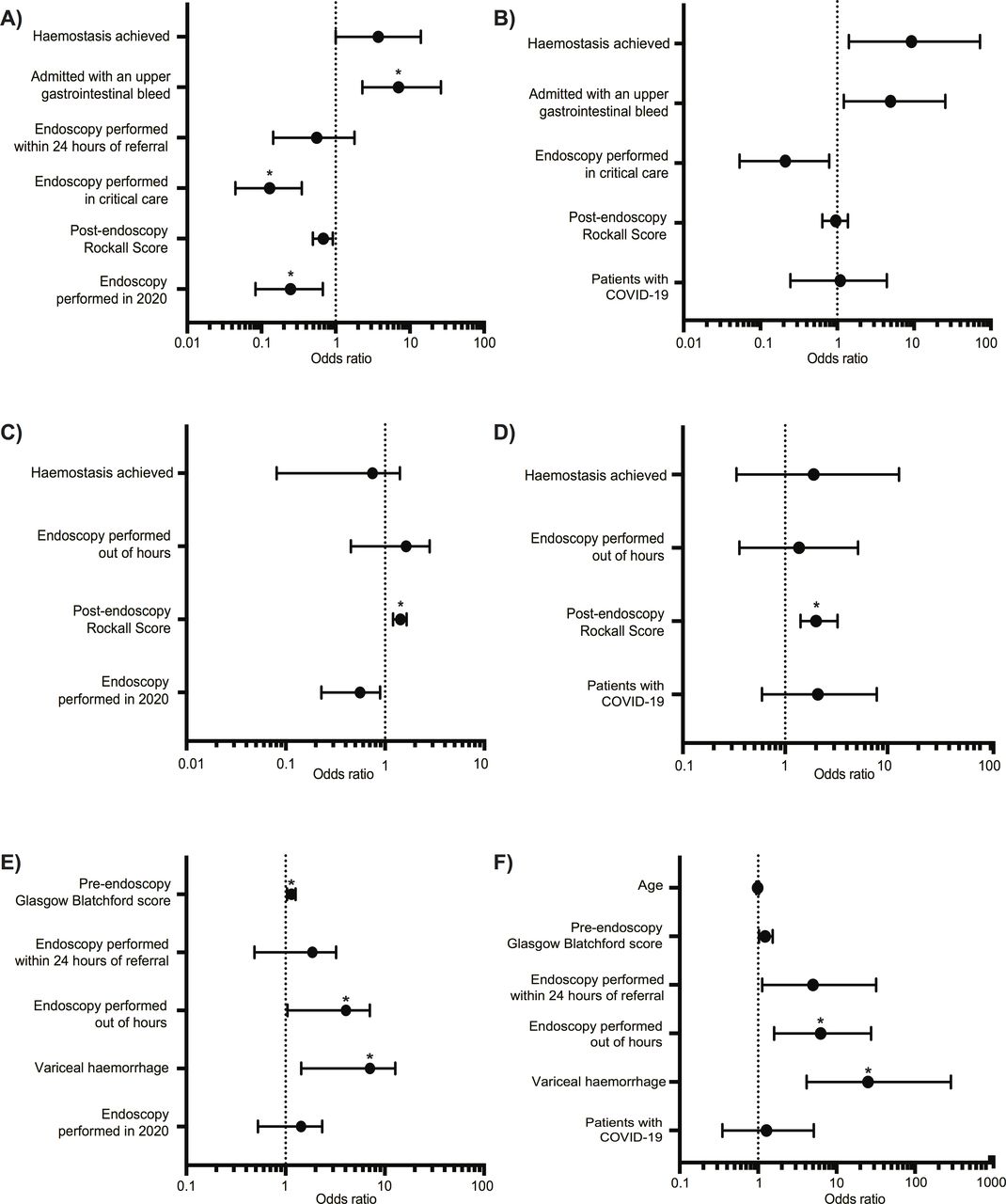
A multiple logistic regression model was used to discern whether endoscopy for UGI bleeds in 2020 was independently associated with a reduced 30-day survival (figure 2A). After adjustment for listed covariates, endoscopy performed in 2020 was associated with reduced 30-day survival (OR 0.25, 95% CI 0.08 –0.67). Within this model, patients who underwent endoscopy on critical care were less likely to survive the 30-day period (OR 0.13, 95% CI 0.04–0.35) and patients admitted with a UGI bleed were more likely to reach 30-day survival (OR 7.04, 95% CI 2.29–26.14).
{kind=link}
{kind=link}
Multiple logistic regression models evaluating the risk of adverse outcomes for endoscopy in the COVID-19 era or patients with COVID-19. OR plots indicating (A) factors associated with reduced 30-day survival in the COVID-19 era (n=221, pseudo R2=0.3498), (B) considerations for 30-day postendoscopy survival in patients with COVID-19 (n=80, pseudo R2=0.2813), (C) factors impacting 30-day major rebleeding in the COVID-19 era (n=221, pseudo R2=0.1523), (D) considerations for a risk of a major rebleeding event within 30 days of endoscopy in patients with COVID-19, (n=80, pseudo R2=0.2541), (E) indicators influencing the likelihood of therapeutic intervention at endoscopy in the COVID-19 era (n=219, pseudo R2=0.2049, (F) factors indicating the requirement for therapeutic intervention at the time of endoscopy in patients with COVID-19 (n=80, pseudo R2=0.3696). *Indicates statistical significance following correction for false discovery.
Following univariate analysis of data from 2020 (online supplemental table 3), a second multiple logistic regression model was formulated to determine whether COVID-19 status impacted postendoscopy survival (figure 2B). No significant relationship was observed between COVID-19 status and 30-day survival (OR 1.10, 95% CI 0.25–4.42).
No difference in risk of major rebleeding observed following endoscopies performed for UGI bleeds in 2020 or in patients with COVID-19
Major rebleeding complicated 91 of 224 (40.6%) endoscopies within 30 days. By univariate analysis (online supplemental table 4), higher GBS (10.8 vs 8.9) and Rockall Scores (5.6 vs 4.1) were significantly associated with a major rebleed. There was a higher rate of intervention (38.5% vs 23.5%) and a lower rate of haemostasis (83.3% vs 94.0%) at the time of endoscopies complicated by a major rebleed. However, these relationships were not significant when corrected for false discovery.
Using data from 2020 and 2019, a multiple logistic regression model was devised to evaluate whether endoscopy in 2020 was associated with an increased incidence of major rebleeds within 30 days (figure 2C). After adjustment for covariates endoscopy performed in 2020 was associated with a reduced incidence of major rebleeds within 30 days (OR 0.50, 95% CI 0.26–0.92); however, this did not achieve significance after correction for false discovery. Given that patients’ deaths and major rebleeds were potentially competing endpoints, the analysis was repeated with non-survivors excluded (online supplemental figure 1A). This demonstrated no association between major rebleeds and endoscopy performed in the COVID-19 era (OR 0.51, 95% CI 0.25–1.00).
Following univariate analysis of data from 2020 (online supplemental table 5), a second multiple logistic regression model was formulated using data from 2020 to discern whether endoscopies performed for patients with COVID-19 were associated with an increased risk of major rebleeds within 30 days (figure 2D). Patients with COVID-19 had a similar risk of major rebleeding compared with patients without COVID-19 (OR 2.14, 95% CI 0.59–7.86). Excluding non-survivors did not reveal a significant association between patients with COVID-19 and major rebleeding (online supplemental figure 1B)
Patients who underwent UGI bleed endoscopy in 2020 or had COVID-19 were not more likely to receive intervention at the time of endoscopy
Out of 223 endoscopies, 66 (29.6%) involved therapeutic intervention. The intervention was more frequent in patients who had endoscopy performed out of hours (34.8% vs 10.3%), those with variceal haemorrhage (31.8% vs 7.7%) and those with higher GBS (11.0 vs 9.1) (online supplemental table 6). There was increased intervention in patients undergoing endoscopy within 24 hours of referral (81.6% vs 67.3%), although this relationship was not significant following correction for false discovery. UGI bleed endoscopy in 2020 was not associated with an increased adjusted risk of therapeutic intervention at the time of endoscopy compared with 2019 (OR 1.24, 95% CI 0.64–2.42) (figure 2E).
Following univariate analysis of data from 2020 (online supplemental table 7), a multiple logistic regression model was used to determine if patients with COVID-19 were more likely to receive intervention at the time of endoscopy (figure 2F). There was no significant association between COVID-19 status and the adjusted risk of interventions (OR 1.28, 95% CI 0.35–5.13).
Discussion
Our findings demonstrate a reduction in UGI bleed endoscopy in the COVID-19 era in concordance with international experience.6 7 To our knowledge, this is the largest description of UGI bleed endoscopy outcomes in the COVID-19 era.
We demonstrate that postendoscopy survival has reduced below the accepted 90% standard in the COVID-19 era.8 9 However, when comparing the 2020 and 2019 cohorts, there are no significant differences in UGI scores pre-endoscopy and postendoscopy. This is important as the Rockall Score and GBS have prognostic value in the management of UGI bleeds with regard to interventional requirement and rebleeding risk.10 11 However, these scores perform relatively poorly when used to predict mortality following UGI bleed, suggesting that patient death is typically unrelated to ongoing GI bleeding.10 This is supported by our findings that under 10% of non-survivors had GI bleeding recorded on their death certificate. Patient comorbidity is a well-described risk factor for mortality post UGI bleeding,12 and although not directly quantified, we recorded age, admission reason and prognostic scores, which account for major comorbidities. Patients experiencing UGI bleeding on critical care units are also known to have increased mortality in comparison with those in general wards.13 We demonstrated that patients who underwent endoscopy for UGI bleeding in the COVID-19 era were at greater adjusted risk of mortality, suggesting that patients presenting late is not the lone reason survival has reduced.
The in-hospital mortality of patients with COVID-19 is reported as 28%–39%14–16 and higher in patients with comorbidities.14 17 18 We found no difference in 30-day postendoscopy survival of patients with COVID-19 compared with those without, although it is likely that our study was underpowered to detect a difference in this cohort.
It is noteworthy that irrespective of COVID-19 status, the 2020 cohort did not have an increased rate of rebleeding at 30 days or endoscopic intervention. Rebleeding is associated with a significantly higher mortality9 and patients requiring endoscopic interventions are more likely to rebleed.19 20 However, the observed rate of rebleeding in the 2019 cohort was 45.1%, which is higher than in other published reports.9 This may be accounted for by the fact that several of these hospitals are regional referral centres for refractory variceal and non-variceal haemorrhage. Previously described associations between rebleeding, the Rockall Score, GBS and need for intervention were observed across both cohorts.21 22 Major rebleeding within 30 days and interventions at the time of endoscopy were not associated with reduced survival in either cohort, nor were there differences between 2020 and 2019 endoscopy secondary outcomes or seniority of the endoscopist. It is therefore unlikely that the reduced 30-day survival in the COVID-19 era relates to either operator or endoscopy-related factors.
The development of a ‘COVID-centric’ health service may have contributed to the increased mortality following endoscopy in 2020. The pandemic placed enormous strain on resource and staffing with specialist healthcare workers redeployed to the ‘frontline’. All units within this study were affected, with medical and nursing staff alike redeployed leaving GI bleed services without the usual support of specialist gastroenterology teams. Undoubtedly, this affected the ability to deliver quality patient care and it is possible that clinician thresholds for UGI bleed endoscopy have increased. Given the fear of a second peak and the current lack of available cure or vaccine, this is an area requiring urgent attention. Pathways require review with consideration of developing COVID-19 minimised and COVID-19 ‘hot’ services that prioritise patient safety, appropriate staffing and PPE to enable patients to receive timely access to emergency endoscopy.23
We acknowledge the limitations of this study; with its retrospective observational design. Outcomes were, however, derived from prospectively entered data and were therefore not subject to recall bias. This study included patients in teaching hospitals and referral centre bias may mean our cohort were more likely to have severe GI bleeds and complications. We were unable to evaluate any potential change in clinician thresholds for performing endoscopy for UGI bleeds. Given the reported incidence of 4%–13.7% for GI haemorrhage among patients with COVID-1924 25 and the London hospital bed occupancy during this time period (figure 1A), it is surprising that only 19 patients with COVID-19 underwent endoscopy for UGI bleeding. This may be due to a reduction in referral for endoscopy in this group due to concerns of their mortality risk or the reluctance to undertake procedures on patients with active COVID-19. There may have been reduced access to critical care for a patient with multiple comorbidities or those with a high risk of mortality in comparison with 2019. Therefore, the use of critical care admission as a surrogate for comorbidity and disease severity must be interpreted cautiously. We note that the PCR test for SARS-CoV-2 indicating COVID-19 does not have 100% sensitivity and therefore there may have been patients in the negative cohort who had COVID-19. We also appreciate that there may be differences between 30-day in-hospital and 30-day overall survival. The Benjamini-Hochberg procedure was used to prevent false discovery, thus our positive findings are highly likely to be valid, conversely, this measure has an inherent increase in the chance of false negatives. Although we suspect the increased mortality is likely to be secondary to the response to the pandemic, we have not been able to directly demonstrate causation and this requires further investigation. The strengths of this study should be recognised; it is a multicentre study using multivariate models to assess variables in the COVID-19 and pre-COVID-19 era. We evaluated objective clinical endpoints of survival, rebleeding and therapeutic intervention. Finally, this is the first study to examine the impact of the COVID-19 era on outcomes in individuals with UGI bleeding.
In conclusion, we demonstrate that post-UGI bleed endoscopy survival was reduced in the COVID-19 era although major rebleeding and therapeutic intervention at the time of endoscopy were not. COVID-19 was not demonstrated to be a risk factor for mortality or complications postendoscopy. The reduced survival observed in combination with the reduced number of procedures performed likely represents a secondary effect of the response to the COVID-19 pandemic, with patients avoiding hospital and reduced resource and staffing limiting optimal patient management. Urgent work is required to encourage the public to seek medical attention when required and to optimise pathways to ensure that the best possible patient care is provided through the ongoing pandemic.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. De-identified participant data is stored on an encrypted password-protected computer in the Institute of Liver Studies, King’s College Hospital. Data is available on request from Dr OD Tavabie at oliver.tavabie@nhs.net.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
B'HH and DJ are joint senior authors.
Twitter @jennie_clough, @IBDdoc
Contributors BH and DG: study supervision and guarantors of the manuscript.ODT, JNC, USG, BH and DJ: study concept & design. ODT, JNC, JB, MB, HM and USG: acquisition of data. ODT: analysis & Interpretation of data; mathematical & statistical analysis. AS, ND, DG, CG, SLP, SD, USG, BH and DJ: administrative/technical/material support. ODT, JNC, JB and USG: drafting of manuscript. ODT, JNC, JB, MB, HM, AS, ND, DG, CG, SLP, SD, USG, BH and DJ: critical revision of manuscript. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.