Article Text

Abstract
Objective Avoiding duodenal biopsy in adults for coeliac disease (CD) diagnosis is controversial. Some retrospective and prospective studies have shown that CD can be reliably diagnosed in adults with serology rather than duodenal biopsies. This study aimed to check the accuracy of a cut-off value of ≥10 upper limit of normal of anti-tissue transglutaminase antibody (anti-TTG IgA) titres for CD diagnosis in adult patients.
Method We retrospectively analysed adult patients (≥16 years) who underwent gastroscopy from 2013 to 2018 for positive coeliac serology. The relationship between titres and disease was determined by using linear models, whereas sensitivity and specificity were assessed by receiver operator curve.
Results We analysed 144 newly anti-TTG antibody-positive adult patients with a median age of 48.5 years (IQR 32–62); among them, 86 (60%) patients had CD (Marsh III: n=68 and Marsh II and I: n=18) with a higher prevalence in females (n=59 (69%)) and Europeans (n=60 (70%)). Fifty (58%) patients with CD had colonoscopy and five (6%) had imaging; only six patients were diagnosed with additional conditions. An anti-TTG IgA titre cut-off value of 150 U/L was 100% specific for CD in our dataset, with 70% (95% CI: 60% to 88%) sensitivity for this patient group.
Conclusion Coeliac serology using anti-TTG IgA with titres ≥10× normal value is an excellent predictor of CD, irrespective of age, gender and ethnicity. Duodenal biopsy may not be necessary in selected adult patients with CD, especially younger than 50 years of age without additional gastrointestinal red-flag signs and symptoms.
- celiac disease
- small intestinal biopsy
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available upon reasonable request. Restrictions apply to the availability of data from JB with the permission of Counties Manukau Health Research Office.
Statistics from Altmetric.com
Summary box
What is already known on this subject?
A ‘no duodenal biopsy’ approach’ is well established in paediatric guidelines for diagnosing coeliac disease (CD). A 10-fold increase in anti-tissue transglutaminase antibody (anti-TTG IgA) levels with anti-endomysial antibody positivity is sufficient to make a diagnosis of CD in the absence of duodenal biopsies. CD diagnosis without duodenal biopsy is deemed controversial in adults because of concerns about missing life-threatening concomitant diseases despite limited evidence for this.
What are the new findings?
Apart from showing that anti-TTG IgA titres of ≥10 times the ULN excellent specificity at detecting CD, we also showed that the presence of life-threatening concomitant disease was rare.
How might it impact on clinical practice in the foreseeable future?
The findings of this study support the approach of serology-based diagnosis of CD in patients without red-flag signs and symptoms. This approach has significant clinical practice implications in the current scenario of the COVID-19 pandemic. It may help to reduce unnecessary procedures and reduce the wait time of more urgent cases in a stressed healthcare system.
Introduction
Coeliac disease (CD) prevalence worldwide is about 1.4% based on serological testing and 0.7% based on biopsy findings.1 However, the majority of CD cases are undiagnosed because of a lack of typical disease presentation.2 3 The prevalence of CD in New Zealand is the highest reported at 1 in 82 people, with 80% of cases being unaware they have the disease.4 5 CD diagnosis is increasing in both young and geriatric populations due to a better understanding of the disease’s natural history, pathogenesis and availability of highly accurate serological tests.6 The diagnostic paradigm for CD changed with the advent of small intestinal biopsies in the 1950s and then through the development of serology tests as screening tools in the 1980s. Serological tests like anti-endomysial antibody (EMA) and anti-deamidated gliadin peptide (DGP) had issues related to the demand for skilled expertise, cost and diagnostic accuracy.7–10 Today the most widely used serological screening test is anti-TTG antibody, which is cost-effective and has both a high sensitivity and specificity.9 10 Duodenal changes in CD are non-specific and can be present in other conditions,11 but still, duodenal biopsy is considered the gold standard for CD diagnosis.12–15 Furthermore, duodenal sampling involves an invasive procedure, resources and risks misdiagnosis if disease is patchy or sampling is inadequate or poorly oriented.9–11 16–19 The accuracy of current serology assays and the correlation at ≥10 anti-TTG antibody upper limit of normal (ULN) titres with mucosal changes is reportedly excellent16–27; therefore, the duodenal biopsy approach for CD diagnosis needs revisiting in the light of current COVID-19 pandemic scenario.
‘No duodenal biopsy’ algorithms are well established in paediatric patients rather than in the adult population.12 15 20 21 However, recently published Finnish national guidelines for the diagnosis of CD and COVID-19-related British Society of Gastroenterology interim guidance for suspected CD have incorporated this diagnostic pathway.28 29 This study aims to identify whether a ≥10 anti-TTG IgA ULN antibody titre is a reliable cut-off value for CD diagnosis that would safely validate a no duodenal biopsy approach in adult patients.
Methods
This is a single-centre retrospective study conducted at Counties Manukau District Health Board (CMDHB). Positive coeliac serology data were extracted from the CMDHB laboratory from January 2013 to December 2018. We included all newly positive anti-TTG IgA antibody adult patients (age >16 years), followed by duodenal biopsy on a normal diet. Paediatric patients, follow-up cases, patients who had duodenal biopsies prior to serology and/or patients who had not had duodenal biopsies at all were excluded from the study. We reviewed clinical records to identify patients’ demographics (age, sex and ethnicity), indications for investigations, comorbidities and time from serology analysis to duodenal biopsy. As well as recording macroscopic features on endoscopic examination and histological findings assessed by using Marsh Criteria,30 we documented the number of duodenal biopsies taken during gastroscopy.
Symptomatic patients with positive serology and Marsh I–III histology scores with improvement on gluten-free diets were categorised as CD according to the recent European guidelines.11 Furthermore, we looked at other investigations performed in the selected cohort for the exclusion of additional diagnoses.
The CMDHB laboratory used the ‘Bio-Rad Autoimmune EIA Anti-TTG IgA immunoassay’ to perform all CD serology testings (normal range ≤15 U/mL; positive range >15 U/mL). This immunoassay has a coating of recombinant human tissue-transglutaminase and gliadin-specific peptides and it is therefore reported to have little cross-reactivity to other autoantigens, and its sensitivity and specificity are reported as 97% and >95% respectively.
Statistical analysis
Categorical values were expressed as a percentage of the sample. Numerical variables were stated as median with IQR. The relationship between anti-TTG titres and disease was determined by using linear models, whereas sensitivity and specificity were assessed by the receiver operator curve.31 We used a multivariate linear regression to look at moderation and interactions between variables and compared competing models using Akaike information criterion (AIC).32 Variables comprised age, gender, ethnicity and CD status.
CD cases may present differently by age, so we grouped presentations by <50, 50–59 and 60+ age classes for analysis. Fisher’s exact test was used to look at overall differences between age classes and binomial proportion CIs calculated. Data were analysed using R.33
Results
We identified a total of 340 patients with positive serology between 2013 and 2018. Only 144 adult patients met the inclusion criteria and among them 86 (60%) had a confirmed CD diagnosis (figure 1). The median age of CD diagnosed patients was 40 (IQR: 24–50) years, with the majority being females (59 (69%)) and of European ethnicity (60 (70%)). The common indications for coeliac serology testing were iron deficiency anaemia (n=52 (36%)), diarrhoea (n=34 (23.5%)), abdominal pain/bloating (n=34 (23.5%)) and weight loss (n=24 (17%)). The median serology to biopsy time was 129 (IQR: 29–209) days. The most common endoscopic finding in patients with confirmed CD was duodenal mucosal flattening and scalloping; whereas, Marsh III was the most common finding on histology. However, endoscopic changes were reported normal in 23 (27%) patients with CD (table 1).
Patient’s demographics and basic characteristics
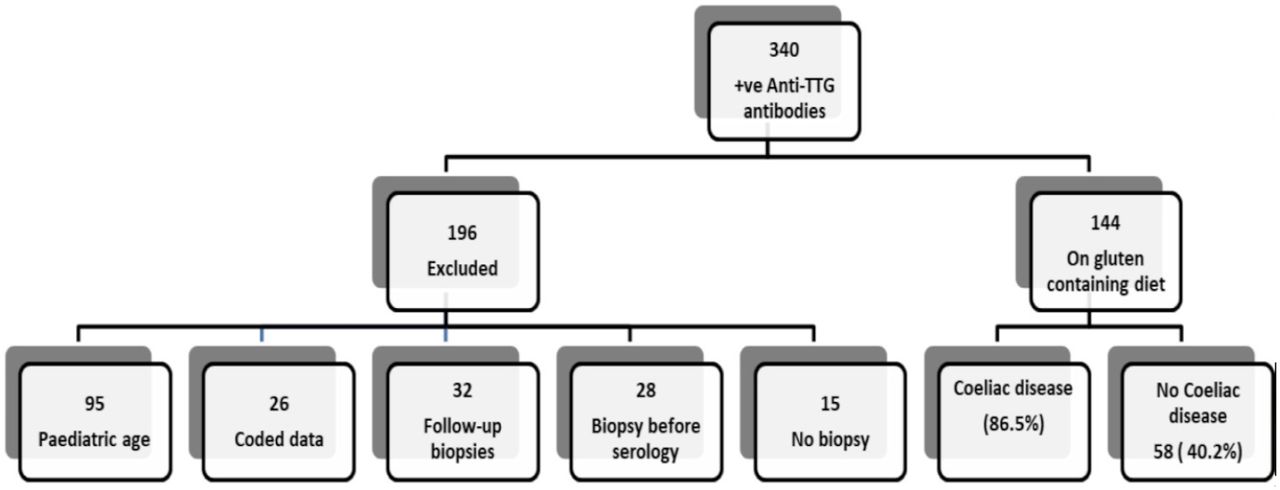
Flow diagram of case selection. TTG, tissuetransglutaminase
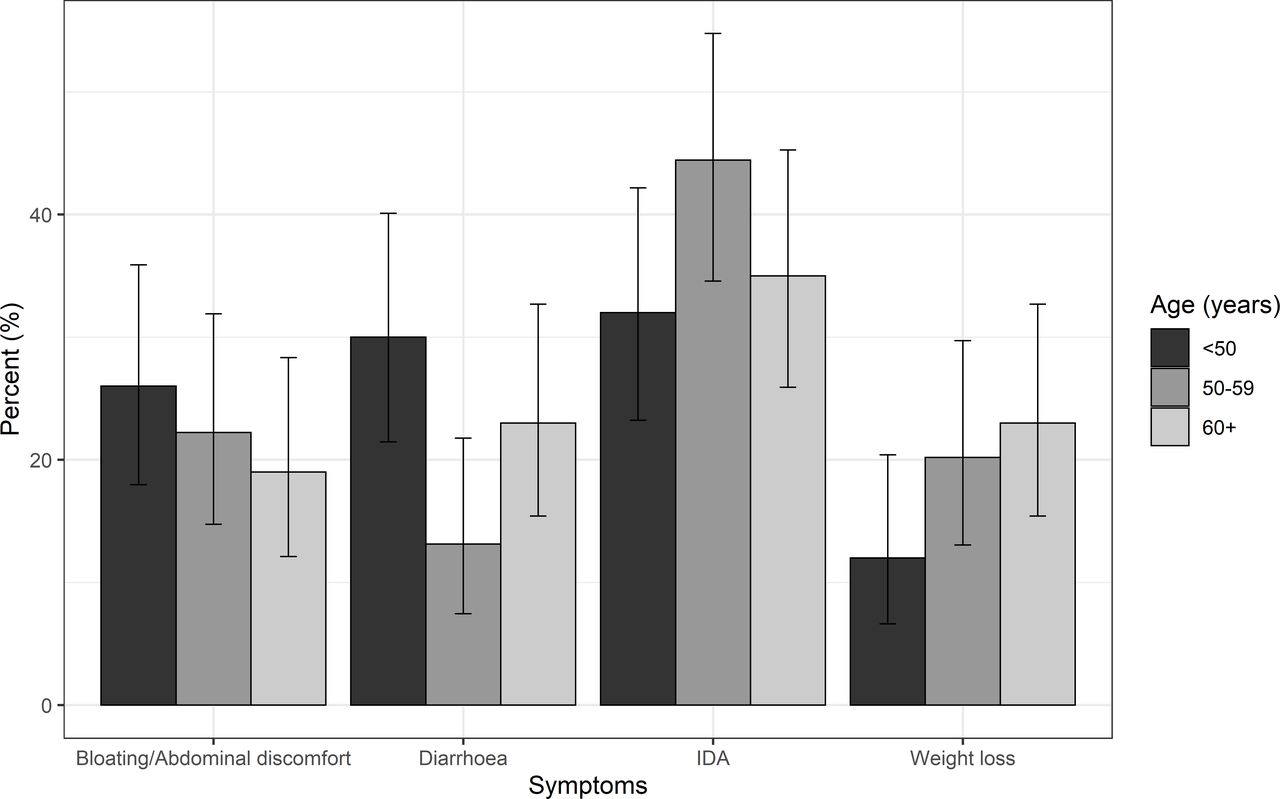
Of 144 patients, 73 (51%) were <50 years, 45 (31%) were between 50 and 65 years and 26 (18%) were >65 years. The symptom presentation was more or less similar across all the age groups (p=0.4). Iron-deficiency anaemia was most common and more prevalent in patients >50 years. Diarrhoea was most common among the <50 age group and weight loss the next most common among 60+ age group (figure 2).
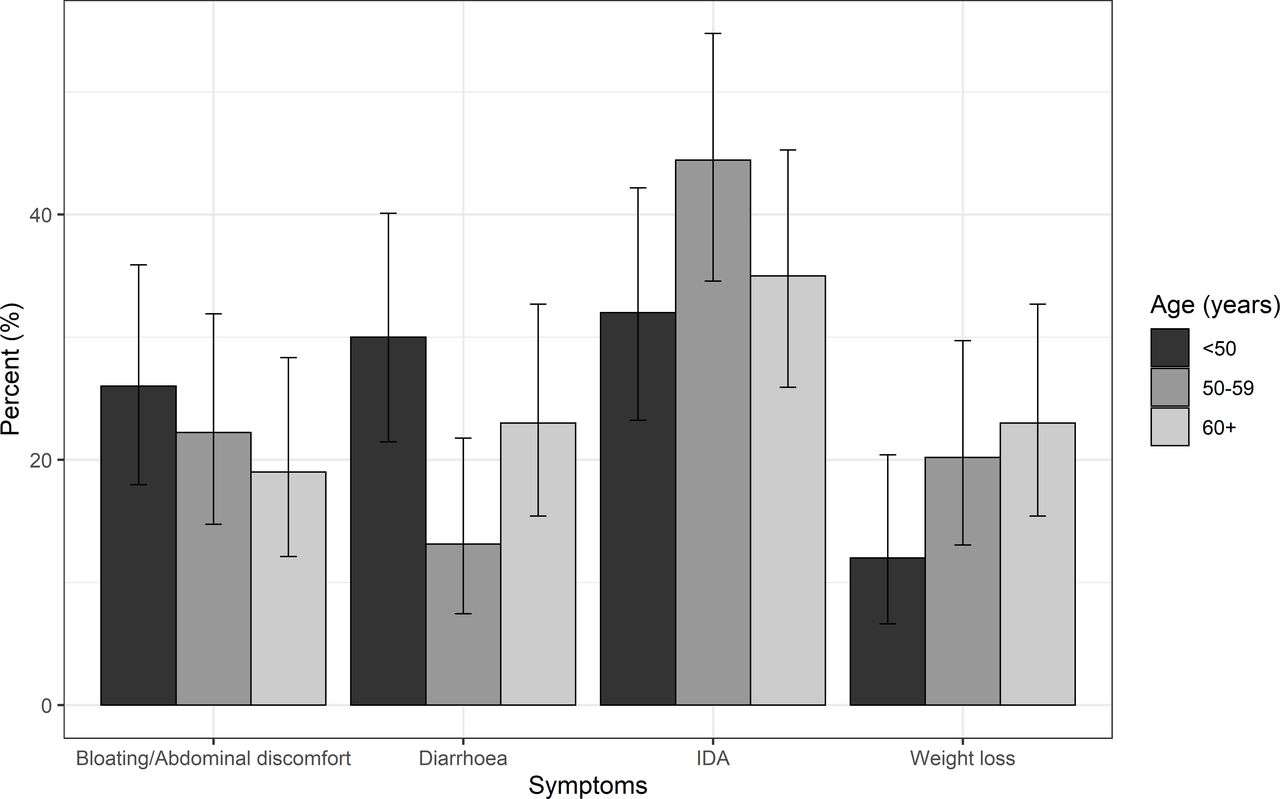
Age-specific symptom prevalence in our sample with 95% CIs. IDA, iron-deficiency anaemia.
Overall, 23 (27%) patients with CD had associated conditions like diabetes, thyroid disease, asthma and other autoimmune conditions. Eighty-eight patients had a colonoscopy; two-thirds of them had a median age of 63 (IQR: 58–70). Of 86 patients with CD, 50 (58%) had a colonoscopy, and 5 (6%) had a CT/MRI; only 5 patients were found with additional diagnoses of inflammatory bowel disease (IBD), small bowel cancer, microscopic colitis and diverticulosis (table 2). The patient with small bowel adenocarcinoma had underlying severe HIV disease.
Further investigations and additional diagnosis in patients who were serology positive (CD)
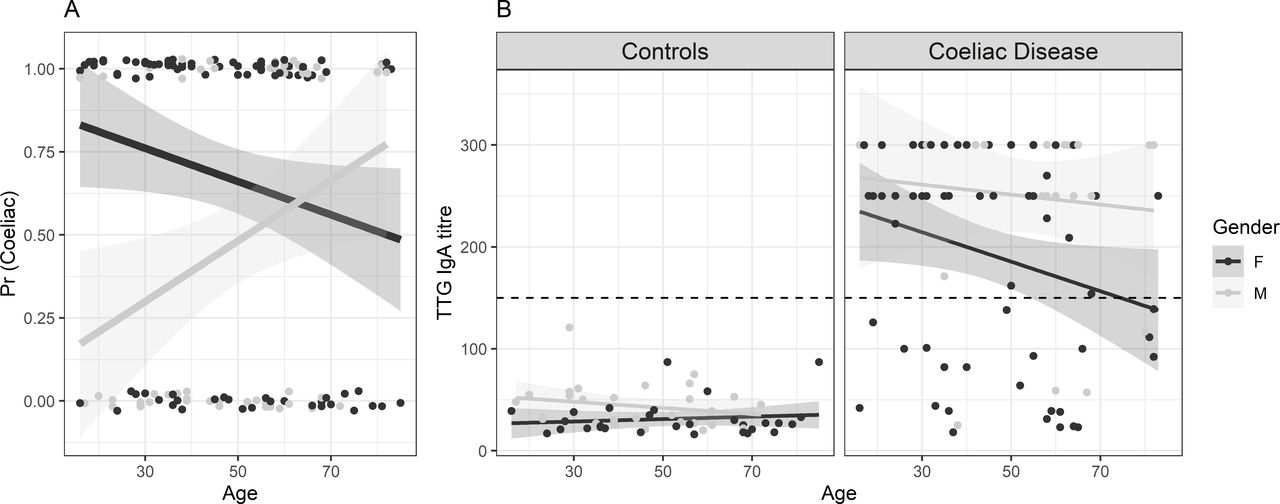
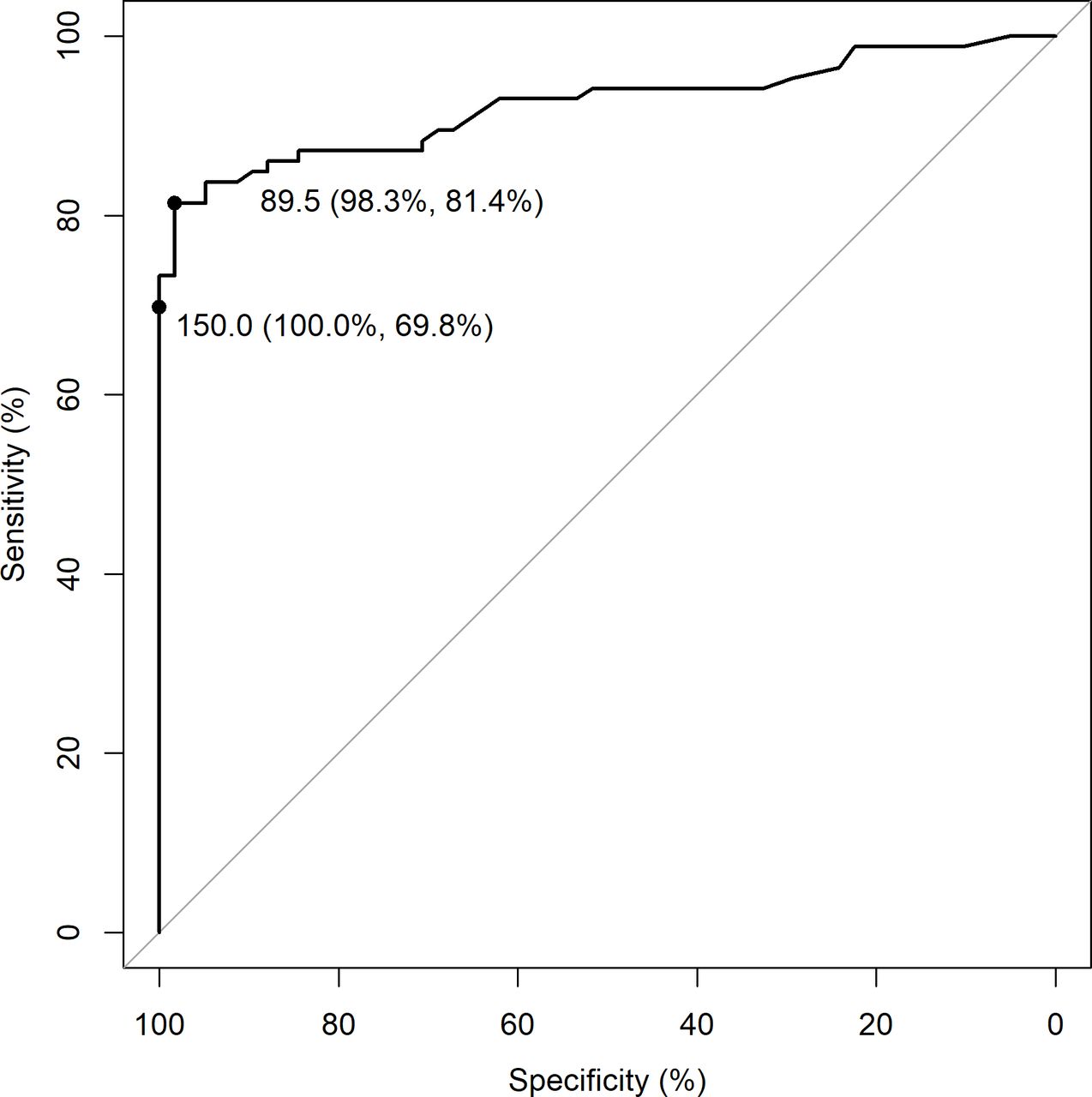
CD was higher in younger females than males, but this difference disappeared beyond approximately 50 years of age (figure 3). In univariate analyses (not shown) there was no difference in anti-TTG IgA titres by age, sex and race. The multivariate regression analysis best model by AIC had age as a factor predicting anti-TTG titres, along with an interaction between gender and CD (see online supplemental material), showing coeliac men had higher anti-TTG titres than women, with titres declining with age (figure 3). Despite these differences, a cut-off value of 150 anti-TTG IgA titre was 100% specific in our dataset for CD. However, the sensitivity was only 70% (95% CI: 60% to 80%). For comparison, the Youden’s optimised titre threshold was 89.5% (95% CI: 57% to 94%). This 89.5 threshold was less specific (84%, 95% CI: 74% to 92%) but had a higher sensitivity (98%, 95% CI: 91% to 100%) and positive predictive value (PPV) (figure 4, table 3).
Supplemental material
Diagnostic test statistics for a 150 titre and the Youden’s optimised titre
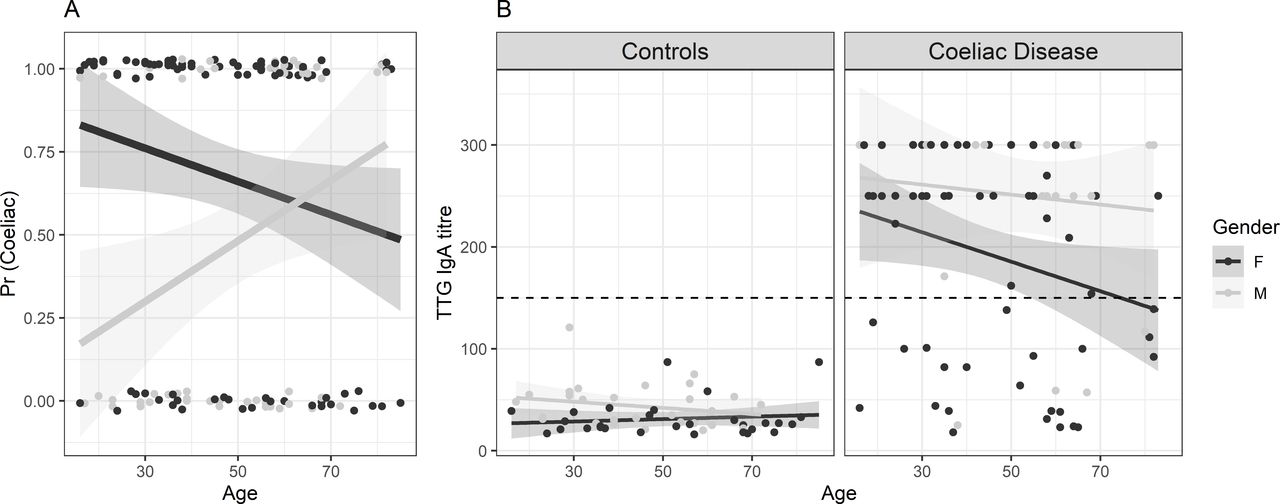
Distribution of anti-TTG IgA titres based on gender and age. (A) Case probability in our dataset. (B) Anti-TTG IgA titres by non-coeliac and patients with coeliac disease, age and gender. The dashed grey line is the 150 U/mL cut-off; dark grey indicates female patients; light grey indicates male patients. TTG, tissue transglutaminase.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Performance of anti-TTG IgA as a predictor of Marsh scores. Specificity and sensitivity are shown in parentheses with the >10 times the upper limit of normal (150) and optimised Youden’s index (89.5). TTG, tissue transglutaminase.
Discussion
Our study supports the reliability of the anti-TTG IgA cut-off value of ≥10 times the ULN for the CD diagnosis in adult patients. A cut-off value of ≥10 times the ULN provided 100% specificity irrespective of age, sex and ethnicity, consistent with previous publications.16–27 The ‘no-duodenal biopsy’ approach is likely safe as life-threatening coexisting diseases were rare in our patients with CD after appropriate risk stratification. Omitting duodenal biopsies is adopted in the European Society of Paediatric Gastroenterology, Hepatology and Nutrition and British Society of Paediatric Gastroenterology, Hepatology and Nutrition guidelines for patients with anti-TGA-IgA values ≥10 times the the ULN.20–22 Several retrospective and prospective studies published after these paediatric guidelines have supported this assertion.18 19 23–27
Similar to endoscopic changes, biopsy results can be inconclusive and non-specific.2 6 Establishing the diagnosis of CD by analysing duodenal biopsies from adults has been considered as the gold standard, despite reports of errors related to biopsy sampling and its interpretation.6 9–11 Approximately 5%–10% of the specimens are uninterpretable because of sampling error or poor preparation.9 16–19 There are also reports of disparity among histopathologists in the interpretation of duodenal biopsies.34 Further, CD presentation has changed significantly in the last six to seven decades, and symptoms of severe malabsorption and complete villous flattening are less frequent. Moreover, the small bowel mucosal changes can be patchy,9 16–18 and these histopathological changes can mimic other conditions like infections (eg, with Giardia lamblia, Helicobacter pylori or various viruses), autoimmune disorders (eg, thyroiditis, type I diabetes mellitus and others), drugs (non-steroidal anti-inflammatory drugs), food intolerance (eg, lactose) and hypersensitivity (eg, gluten sensitivity).11
In the last two to three decades, the standard of serological testing for CD has improved significantly. The new generation serological kits have high sensitivity and specificity. In the ProCeDE prospective multicentric study, seven out of nine different serological kits used had a PPV of 100% with titres of ≥10 times the ULN and some at even lower levels. Only 0.56% (4/707) of patients had a false positive test with titres of ≥10 times the ULN. The recommendation of titres of 10 times the ULN is considered appropriate for the non-biopsy approach because of interlaboratory and intralaboratory variability and the lack of standardisation.25
The incidence of CD was 3 per 100 000 person per year, less than observed for the population size in this study, despite a high prevalence of CD in New Zealand.4 This inconsistency may be because of two reasons. First, our study population in CMDHB was predominantly Pacific, Maori and Asian (60%), whereas the rest of New Zealand is European dominant (70%). Second, we included positive serology only from our hospital laboratory, given significant variability in community serology tests. Consistent with the previous studies, CD diagnosis here was higher in females younger than 50 years.35–37 Gender and age affected the anti-TTG IgA titres in multivariate regression modelling without impacting a cut-off value to achieve 100% specificity. These differences can be due to the natural history of disease, that is, physiological or immunological differences.38 39
A no duodenal biopsy approach not only eliminates potential complications of gastroscopy but importantly saves healthcare cost and avoids management delay, which was more than 3 months in our study. The no duodenal biopsy approach in patients without red-flags symptoms, such as bloody diarrhoea, dysphagia, severe weight loss and age >50 years, could significantly reduce unnecessary endoscopy procedures in about 50% of patients with CD.15 24
In this study, 28 patients with CD had coexisting diseases, the most frequent being thyroid disease and diabetes, which is more or less consistent with previous studies.40 There is an association between CD and small bowel malignancy, but its prevalence is 0.5–1 per million people, and usually evolves in patients with refractory CD and patients with underlying risk factors, like familial polyposis syndrome, IBD and HIV infection, as was the case in our diagnosed patient.6 40 41 The high colonoscopy rate in this study was presumably because of the predominantly older composition of the study cohort with red-flag symptoms and signs.
A no duodenal biopsy approach lacked support in the adult population previously, because of several reasons: (1) concerns of missing concomitant disease or malignancy, (2) establishing the diagnosis with certainty, (3) its prognostic value as a reference for comparison and (4) being a minor procedure in comparison to the paediatric population.24 25 42 Current guidelines suggest screening for alternative diagnoses in all subjects with CD, which does not necessarily require duodenal biopsies.12–15 Small intestinal follow-up biopsies would not help in a significant proportion of patients, given villous flattening persists for more than 12 months in 50% of patients, and in 10% will never heal.43–45 A follow-up biopsy should be reserved for patients suspected to have rare complications like refractory CD or suspected upper gastrointestinal malignancy. Refractory CD diagnosis is a clinical diagnosis with severe histological changes despite being on a gluten-free diet and so a baseline biopsy would not be helpful anyway.24 25 42
The strengths of this study are the completeness of our data through access to comprehensive records and the excellent length of follow-up. Alternative and additional diagnoses have been excluded in most of the patients. All patients have validated serological testing from the same central laboratory.
However, there are some limitations to the design. This is a retrospective study with no recruitment of patients with positive serology from community laboratories for comparison. There was no EMA and human leukocyte antigen (HLA) status available for most of the patients, though HLA typing is not considered mandatory for CD diagnosis because of its low diagnostic capability, high cost and limited availability.22 24 HLA typing is mainly used in borderline cases rather than excluding the diagnosis. The predictive capacity of the non-biopsy approach improves with being EMA positive, although EMA testing is not done routinely in many centres because of its high costs, labour-intensive and the interpretation variability.9 46 47 Alternative strategies like simultaneous anti-TTG IgA titre measurement or testing for DGP are therefore being studied to integrate into a no duodenal biopsy algorithm.24 45 46
The impact on the accuracy of the correlation between the serology results with small bowel mucosal changes because of the 3-month delay to biopsy will probably be minimal given histological improvement may take years, even on a gluten-free diet. In some patients, improvement is incomplete, as reported previously.43 44 48 No information was available about the amount of gluten that may have affected histology changes.
Lastly, Marsh I–II is considered less specific for CD; however, our patients with Marsh I–II had anti-TTG titres of ≥10 times the ULN (median 250 U/mL). In the context of strongly positive serology and improvement on gluten-free diet, we had no doubt about a diagnosis of CD in these cases. Despite a range of differential diagnosis, Marsh 0–III can be a feature of CD. Similarly, five patients in a recent study by Penny et al 24 had anti-TTG IgA titres of ≥10 times the ULN without detectable villous abnormalities and they were given a diagnosis of CD based on their strong serology and clinical behaviour.24
We conclude that the case for a no duodenal biopsy approach to CD diagnosis in the adult population is strong with appropriate risk stratification of patients. The aim is not to completely abandon the duodenal biopsy, but to provide a pragmatic approach. This approach will help in cost reduction and decrease the case burden for endoscopic services, especially in the current scenario of the COVID-19 pandemic. Above all, a no duodenal biopsy approach prevents unnecessary delay in the management of patients with CD, as life-threatening concomitant pathologies are extremely rare in the CD population. The concern of misdiagnosis can be mitigated by screening and regular follow-up. Thus, patients <50 years old without red-flag symptoms and signs would be appropriate for the no duodenal biopsy approach for CD diagnosis with an anti-TTG IgA value ≥10 times the ULN.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available upon reasonable request. Restrictions apply to the availability of data from JB with the permission of Counties Manukau Health Research Office.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by Counties Manukau Health Research Office under registration number 1234. All identifiable medical information was anonymised.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors made significant contributions to the design, acquisition of data, analysis and interpretation of data. All took part in drafting and revising the manuscript. All authors read and approved the final manuscript. JB collected data, analysed the data and wrote the manuscript. KR provided the idea for the study and assisted in reviewing the manuscript. SH helped in data collection. DH did the statistical analysis and manuscript editing. SG provided data and helped in manuscript editing. RO supervised the study and assisted in manuscript editing.
Funding DTSH is funded by Royal Society Te Apārangi, grant number MAU1701.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- UpFront