Article Text

Statistics from Altmetric.com
Background
The COVID-19 pandemic has placed extraordinary demands on healthcare services worldwide. Strategic planning for acute COVID-19 care has, during the peak phase of the pandemic, rightly overshadowed the provision of diagnostic services, which have been further restricted by the need to minimise viral transmission to reduce the attendant risks to patients and staff. The risk is compounded by the asymptomatic phase of COVID-19 infection1 and is particularly important in relation to GI endoscopy, given the aerosol-generating nature of many endoscopic procedures.2–4
The British Society of Gastroenterology released early guidance to assist local teams in prioritising certain indications for GI endoscopy, even during the tight restrictions demanded by the peak phase of the pandemic.2 Other endoscopy societies or expert groups have also published guidance on the management of GI endoscopy during the pandemic, and these are summarised elsewhere.5
In the deceleration phase of the pandemic, as defined by a sustained fall in new infectious cases over 14 consecutive days,6 7 healthcare systems will rightly look to implement measures to safely restart activity. Endoscopy capacity should be restored as far as possible while ensuring mechanisms are in place to reassure and protect patients and staff from avoidable risk.
There is significant risk in continued delay of diagnostic services. For GI endoscopy, this relates to cancers as well as other time-critical conditions such as IBD. While COVID-19 has tragically accounted for over 200 000 reported deaths by the end of April 2020,8 there were around 18 million cases of cancer worldwide in 2018 and 10 million cancer deaths, with colorectal and gastric cancer accounting for 17% of deaths.9 It has been conservatively estimated that delays to cancer diagnoses and treatment could be responsible for nearly 7000 additional deaths in England and over 30 000 deaths in the USA.10 It is important that the effects of the pandemic on outcomes from other diseases are mitigated as much as possible to reduce the pandemic’s effect on all-cause mortality.
Data from the National Endoscopy Database indicate that total endoscopic activity fell rapidly to 5% of normal levels during the peak phase of the COVID-19 epidemic in the UK (from approximately 35 000 reported procedures per week to 1700, for the week ending 13 April.11
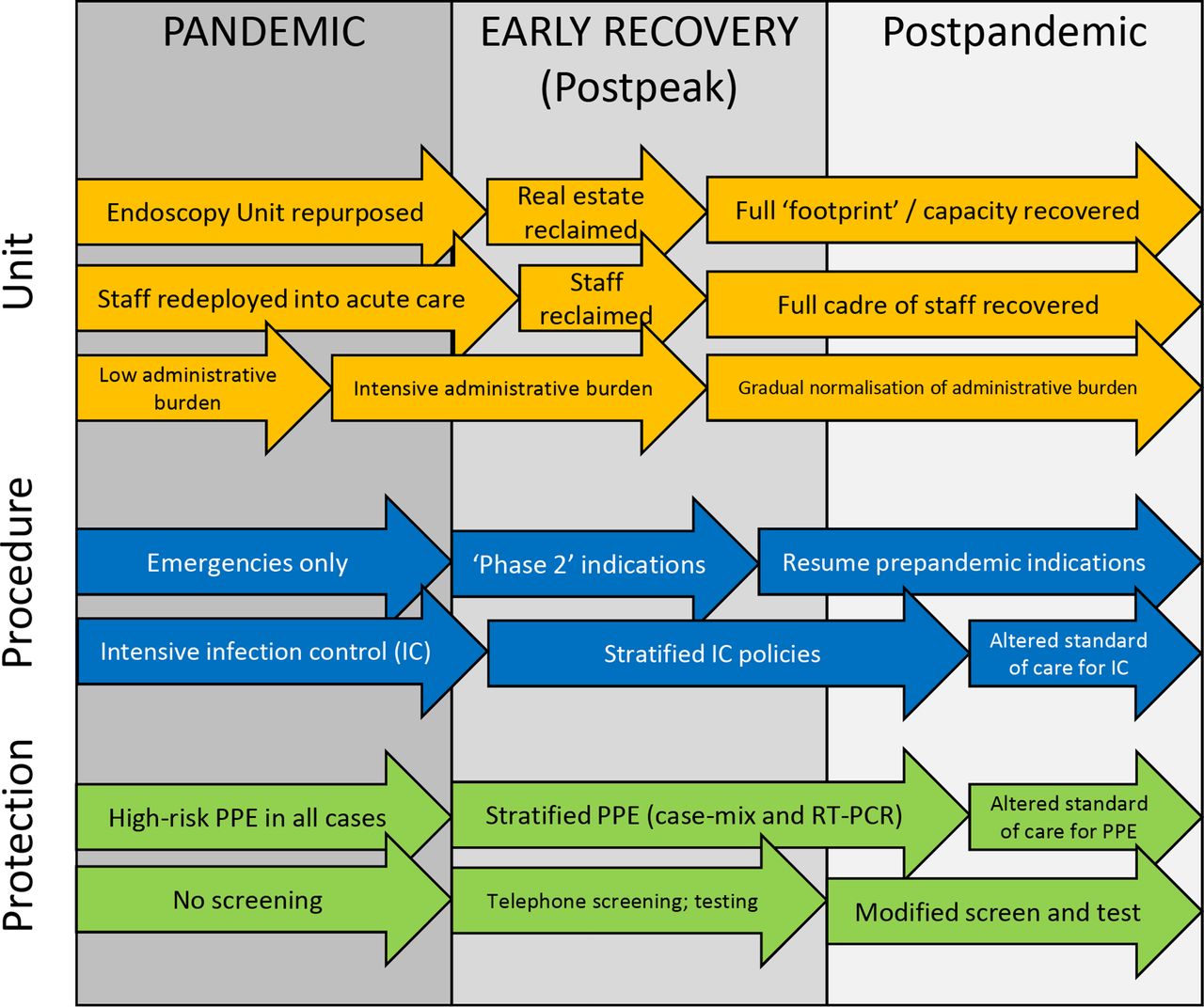
Restarting non-acute activity in a recovery period is crucial but characterised by progressive challenges and considerations with a number of predictable common factors (summarised in figure 1).

Challenges and considerations for restarting endoscopy. This is not intended to be an authoritative list but merely to illustrate key concepts and issues, suggesting possible phases and considerations for strategic planning. Clinical decision-maker support should be added to administrative pathways in the pandemic and early recovery stages. Consideration should be given to service and job plan redesign to facilitate this input in the postpandemic phase. PPE, personal protective equipment; RT-PCR, reverse transcriptase PCR.
The overarching issue will be how endoscopic activity can be resumed at sufficient volume to meet demand, when many services were already under considerable pressure prepandemic.
The first consideration, outside the scope of this article but covered elsewhere,12 will be to ensure robust mechanisms for managing demand and prioritising clinical need. The principles underlying this require senior decision-makers to prioritise based on clinical urgency, developing strategies to match demand with capacity and adjusting that over time as capacity increases. In this article, we seek to outline challenges and suggest recommendations, with a particular focus on screening and testing for COVID-19, to support a gradual resumption of endoscopic activity.
Three broad categories of concern surround the performance of endoscopic procedures for patients in the early recovery and postpandemic phase. These divide into patient factors, procedural factors and infection prevention and control (IPC) strategies, including the appropriate use of personal protective equipment (PPE) (figure 2).

Considerations underpinning endoscopy strategy. *‘Sites’ does not necessarily refer to geographically separate units (eg, separating patients by session or day). LA, local anaesthetic; PPE, personal protective equipment.
Patients may be unwilling to attend hospitals as they perceive that the risk of contracting COVID-19 is high even in an outpatient or ambulatory setting. There are now early reports of patient being unwilling to attend hospitals for procedures during the pandemic.13 Further, patients may be in a designated ‘shielded’ category.14 Approximately 1.28 million such patients in the UK have been advised to self-isolate due to pre-existing medical conditions or current medication, in order to avoid COVID-19 infection. This advice, while lowering their risk of exposure to COVID-19, will put them at greater perceived or actual risk of coming into a hospital environment, thus heightening concern.
Procedural factors must also be taken into account. A new prioritisation stream with appropriate triage and vetting is required, with appropriate planning of staff and operator expertise. Training for those learning endoscopy will be affected and staff will need time to adjust to new operating procedures. Strategies to deal with the impact on training are beyond the scope of this document but are urgently needed.
If all procedures were to be conducted in full PPE and units were to adhere to strict patient flow and IPC recommendations for room cleaning,15 16 their capacity would be severely curtailed (definitely by more than 65%17). This poses a significant challenge and, even in the short term, universal application of maximal infection control strategy is unsustainable.
When considered together, these factors are underpinned by a single need: to know whether patients have, or have recently had, COVID-19 and thus to establish whether they may therefore transmit the disease to other patients or staff. This knowledge would allow the development of sites or services stratified by COVID-19 risk, allowing some to perform higher volume endoscopic activity where the risk of infection is low and vice versa. Understanding regional and international rates of infection is also important as risk will vary, depending on COVID disease prevalence. A robust COVID-19 screening strategy should allow as much endoscopy as possible to be delivered in an environment which uses PPE in a correct and manageable fashion.
Strategy for resuming endoscopy services
We propose a strategy defined around five principles: to select patients by procedure, screen them for potential COVID-19 and separate activity streams based on these considerations, then to perform the ‘scope’, followed by surveillance after the procedure at 7 and 14 days for the development of COVID-19 symptoms (figure 3, termed the ‘5S’ principles).

‘5S’ principles outline an approach for restarting endoscopic activity POC. POC, point-of-care; SCOTS, symptoms of infection, close contact with known or suspected cases, occupational exposure (actual or estimated), travel history and ‘shielded’ category.
This approach opens up the possibility of developing ‘COVID-minimised’ or ‘cold’ sites, to serve patients (confirmed to be free of active infection) undergoing low-risk endoscopy, as well as to provide a safer environment for patients who might be considered at higher risk if they were to be exposed to infection.14 The specific IPC policies governing such an approach are likely be hospital-specific, although some standards could be developed at a national level.
Finally, there will be a considerable new administrative burden to support any such initiative. Adequate staffing, including clinical decision-maker support, is axiomatic.
‘Select’: patients, endoscopists and tests
The British Society of Gastroenterology has published guidance to support units to appropriately select patients12 for endoscopy in the recovery phase, which will include allocating appropriate endoscopists and assistants and ensuring availability of equipment. While robust triage mechanisms will be required in the early stages of recovery, to allow patients at greatest need or risk to be prioritised, as infection rates subside and the postpandemic phase progresses, triage may return to prepandemic patterns (figure 1). These considerations are outside the scope of this article and will depend on how healthcare services are organised and delivered and will include, but will not be limited to, vetting and prioritising and using non-invasive tests (eg, faecal immunochemical tests or faecal calprotectin). The role of alternative, less invasive diagnostic tests (eg, video capsule or radiological imaging) might also be considered, but prospective study is required to establish whether these will be safe and cost-effective strategies compared with endoscopy.
‘Screen’: symptom-based
The first step of determining whether any given individual has COVID-19 is to check for symptoms. The incubation period of the disease is estimated to be around 5 days, with the overwhelming majority being diagnosed within 14 days (<1% outside this time frame).18–20
Much has been made of the rate of asymptomatic carriage, with potential for transmission by people unaware that they have the disease.21–25 Reported rates vary considerably, and this might be explained, at least in part, by omission of certain less common or less well-recognised symptoms (at least in the early phases of the pandemic) in these studies. For instance, GI symptoms, particularly diarrhoea, are potential sole manifestations of COVID-19 in a proportion of cases and may be under-recognised.26–29 A further reason to overestimate asymptomatic carriage may be a delay in symptom onset. An outbreak at a skilled nursing facility in Washington State where, although the asymptomatic rate was 27/48 (56%), 24/27 of those residents had developed symptoms within a median of 4 days of the positive test.30 This is in keeping with the known phenomenon of viral shedding from the nasopharynx prior to symptom onset.31
One credible estimate for asymptomatic carriage is from the Diamond Princess cruise ship, where passengers were strictly quarantined from 3 February 2020 and more than 3000 tests were performed (ie, most undergoing more than one test).32 By 20 February, data demonstrated that asymptomatic carriage was at 18%.
The FTOCC criteria , or fever of >38°C, travel to at risk areas, occupational risk, contact exposure and cluster exposure, were developed in Hong Kong to conduct screening during respiratory viral outbreaks (ie, avian influenza and severe acute respiratory syndrome)33 34 and have been proposed in endoscopy preparedness guidelines covering the current pandemic.3 The applicability of these criteria in the context of COVID-19 is not known. The differing nature of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection from other respiratory viruses, in particular, additional symptoms reported,26 27 calls for a broader symptom screen. The FTOCC criteria do not take into account individual patient risks (such as the shielded category), and cluster analysis may prove challenging in varied healthcare systems not geared to this approach.
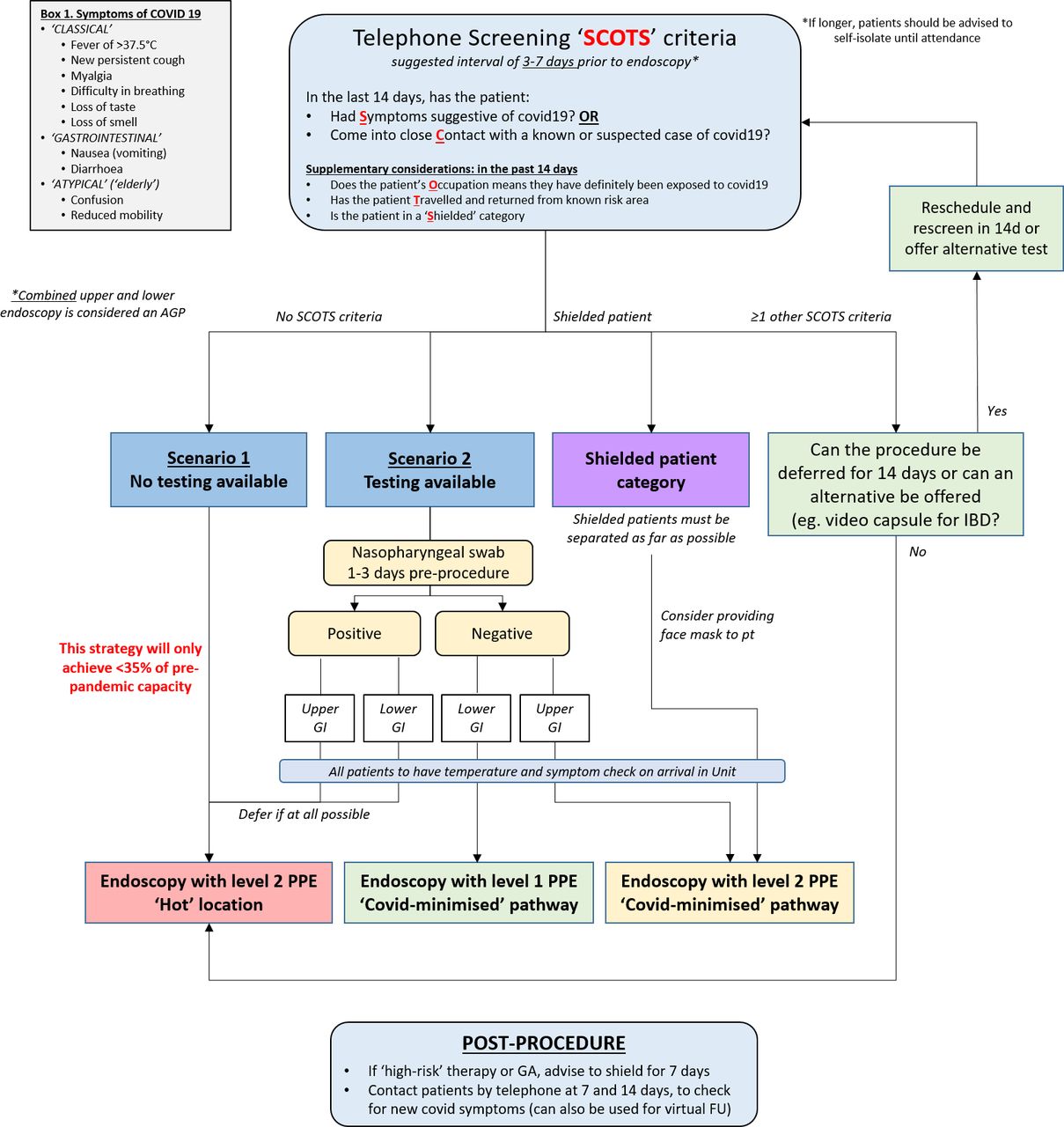
We propose a simplified set of criteria (figure 4) which we have termed ‘SCOTS’. These are based on the core epidemiological principles of symptomatic, infected, exposed, recovered,35 and build on the FTOCC criteria, as well as taking into account patient risk due to pre-existing conditions. A remote (telephone or digital) questionnaire can be applied to enquire about the preceding 14 days for symptoms of infection (which are detailed separately); close contact with known or suspected cases; an occupational exposure (actual or estimated); travel history (ie, to countries or areas with high levels of confirmed cases; this is less relevant in the context of the peak phase and country-wide restriction on travel); and finally, to take into consideration whether the patient in question is in a shielded category.14 If patients answer yes to any one of these criteria, consideration should be given to delaying their planned appointment, depending on clinical urgency.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
‘Screen and scope’ algorithm with SCOTS criteria. AGP, aerosol-generating procedure; FU, follow-up; GA. general anaesthetic; PPE, personal protective equipment; pt, patient; SCOTS, symptoms of infection, close contact with known or suspected cases, occupational exposure (actual or estimated), travel history and‘shielded’ category.
If a patient is in the shielded or ‘occupational risk’ category, endoscopy would not necessarily need to be deferred, but a detailed risk and benefit assessment should be carried out. Particular care should be taken to ensure separation and protection are maintained. Options may include offer of an alternative investigation if clinically appropriate; physical separation and provision of PPE to the patient as well as staff, ideally before travel but certainly before entry into the endoscopy unit; or deferment of the procedure until a later postpandemic stage. The SCOTS criteria should be applied at a reasonable interval from screening to endoscopy appointment (eg, 3–7 days) to allow sufficient time to plan further evaluation and schedule or cancel appointments and to ensure patients do not commence bowel preparation unnecessarily. It is prudent to instruct patients to self-isolate as far as practicable before their planned procedure and a short interval would facilitate this. The symptom-focused questions should be repeated on arrival at the endoscopy unit, where patients’ body temperature should also be checked.
Screen: test-based
Nasopharyngeal swab sampling for reverse transcriptase PCR (RT-PCR) is the mainstay of most COVID-19 testing programmes worldwide. However, published data from which true sensitivity and specificity can be calculated are sparse and of low quality.36 A reasonable indication comes from a series of 51 patients from China with confirmed chest CT findings of COVID-19, where sensitivity of RT-PCR was 71%, while a meta-analysis (with high heterogeneity) suggested a pooled sensitivity of 89% (95% CI 81% to 94%, I2=90%).37 The specificity of RT-PCR is characteristically high,38–41 but a conservative approach would be to use 70% sensitivity and 98% specificity. If prevalence is set at 3%, 10%, 20% and 50%, the negative predictive value (NPV) of RT-PCR then ranges from 99%, 97% and 93% to 77%, respectively (calculated with GraphPad; California, USA). Current estimates of prevalence around the European Union (as of 25 March 2020) are at 82.1 per 100 000 populations with the highest reported in Luxembourg at 323.8/100 000.42 The % of total population infected in the UK is estimated at 2.7% (1.2%–5.4%).43 Even with seven times higher prevalence than currently estimated, therefore, the NPV of RT-PCR is above 90%. Coupled with a negative symptom screen on two occasions, this should serve to reasonably exclude the vast majority of potentially infectious patients from being inappropriately admitted to the endoscopy unit.
Point-of-care (POC) testing has been proposed as a possible solution for rapid test turnaround to facilitate endoscopy. Currently, only one POC test had been licensed by the US Food and Drug Administration (Xpert Xpress SARS-CoV-2 test; Cepheid, USA),44 and a recent assessment of available POC tests by the UK National COVID Testing Scientific Advisory Panel concluded that none had sufficiently good diagnostic performance for clinical use.
At present, the role of antibody testing is still to be established. Optimal tests are still to be determined and availability is limited. When available, antibody testing will prove to be important.45–47 The objective of testing in the context of elective procedures is to prevent patient-to-patient or patient-to-staff transmission (as well as staff-to-patient), but it is unlikely that active infection could be detected reliably by serology, as early reports of sensitivity are low (although higher if performed early enough in the disease stage). Antibody testing may become useful for staff, but concerns have been raised in that, although likely, immunity cannot be assumed even in recovered individuals with positive serology.48 49 Vigilance must be high for active infection in staff scheduled for work and is discussed later.
Chest CT has been suggested by some as a potential screening strategy,17 but the validity and clinical safety of such an approach have been called into question for general population screening and outside of areas of high prevalence38 and cannot be recommended as part of a routine strategy.
Adoption of the ‘screen and scope’ strategy (figure 4) is intended to support the safe resumption of endoscopy services at a reasonable scale. This approach involves applications of the SCOTS criteria before endoscopy and before bowel preparation commences (where it is required), nasopharyngeal swab testing for asymptomatic patients, temperature measurement and symptom recheck on arrival into the endoscopy unit, then proceeding with endoscopy. This will allow case-appropriate PPE to be worn by staff (and the patient if in a shielded category). These proposals are in line with previously published Asian Pacific Society for Digestive Endoscopy and European Society for Gastrointestinal Endoscopy position statements.3 4
‘Separate’: linear patient flow and COVID-minimised units
Systematic identification of patients at the lowest risk of having active infection, as well as those at highest risk if they were to become infected, forms the basis of the next phase of our proposed 5S strategy: separation.
Linear patient flow through the endoscopy unit has been an established principle in GI endoscopy for some time, with limited overlap of pre-endoscopy and postendoscopy patients and ‘clean’ and ‘dirty’ sides of decontamination areas. An additional consideration is required for COVID-19, which separates patients as much as possible, minimising the risk of transmission. Where possible, therefore (and if the physical environment allows), units should consider planning a one-way flow through the department with a separate entrance and exit.5 50
The linear flow model should ensure physical distancing, but careful attention must be given to appointment times and list scheduling to ensure that patients are booked in such a way that more than one patient do not arrive at the same time. Patients should be encouraged to attend at specified times and not arrive early. Relatives or accompanying persons should not attend with patients other than where absolutely necessary, and contact should be minimised when these individuals collect patients after recovery. Slowing the patient sequence with careful spacing should avoid patients being together in waiting areas either preprocedure or postprocedure. Ideally, patients should be held in separate rooms or cubicles rather than in communal waiting or recovery areas. This could mean changes to existing room usage or a change in layout to accommodate more capacity for arrivals, registration/preassessment and recovery. Such considerations will obviously depend on unit size, case mix and local policies. This will be another rate-limiting step in unit capacity, but the creation of COVID-minimised workstreams is a primary concern to ensure safety.
A protocol to allow concomitant swab testing for future scheduled patients, while proceeding with endoscopy for others, potentially in the same unit, may be needed, or it may be possible to consider testing off-site or outside of the endoscopy unit.
The model of a completely separate COVID-minimised unit is an attractive solution to reduce the risk of transmission and to reassure patients and staff. For smaller endoscopy units or in areas which have few units in their region, this may not be logistically possible. In this situation (where the same unit has to be used for low-risk outpatients and much higher-risk inpatients or patients with known COVID-19 undergoing procedures that cannot be deferred), separating the patient stream in time and space should be implemented. One way to achieve this would be to split the unit into COVID (inpatient) and non-COVID (outpatient) sections which do not connect physically, and pathways do not cross, as seen in Prince of Wales Hospital, Hong Kong.5
If this is not possible, then scheduling low-risk outpatients on morning lists and higher-risk inpatients in the afternoon, followed by unit deep cleaning, is an option. Furthermore, ensuring a separate room is available for known high-risk patients or patients with COVID-19 is prudent. Should this be impossible then, for less acute situations, separation of cases by whole-day activity could be an option. This may prove challenging if emergency cases are to be accommodated. A further solution would be to undertake endoscopy in another setting, for example, at the bedside or in an operating theatre designated for infected patients.
‘Scope’: procedure risks and PPE
Much of the risk of risk of COVID transmission has focused around aerosol-generating procedures (AGPs). Upper GI endoscopy (including endoscopic retrograde cholangiopancreatography (ERCP)) is widely regarded as an AGP, with transmissible virus demonstrated in airway secretions.31 The use of throat spray is likely to further exacerbate aerosol generation, but the use of Entonox is not considered an AGP by the Royal College of Obstetricians and Gynaecologists.51 The risk for lower GI endoscopy (flexible sigmoidoscopy and colonoscopy) is less clear, although some guidelines have classified colonoscopy as an AGP.2 3
The transmission of viable virus in stool from asymptomatic carriers has been a subject of considerable uncertainty and debate. The evidence is still evolving, but conclusions can be made to inform practice in the current phase. Multiple studies have demonstrated positive RT-PCR in stool several days or even weeks after respiratory samples become negative.52 There is evidence to demonstrate that SARS-CoV-2 can infect human intestinal epithelium in vivo, although in only one patient,53 and in vitro using a well-established organoid model.54 This was to be expected, given the relatively high expression of ACE2, the functional receptor for the virus, in the human intestine,55 but does not prove transmissibility. The question remains, therefore, whether RT-PCR positivity translates to the presence of viable virus and whether this then indicates a transmissibility risk. In the respiratory tract, this does not appear to be the case. The latter is also probably dependent, to some extent, on viral load in the ‘transmitter’.56 Although a reasonable expectation, it is currently unproven whether COVID-19 transmission risk is dependent on inoculum size.57
A small, but detailed series indicated that, while viral RNA could be detected in stool, viable virus was not present.31 A further small study confirmed this and showed that newly synthesised virus is rapidly inactivated by human colonic fluid.58 This is in keeping with known viral dynamics from sputum and lung aspirates for SARS-CoV-2, where multiple studies have shown no viable virus beyond day 7, while RT-PCR remains positive for much longer, perhaps up to 40 days.52 For SARS-CoV-1, as a comparison, RT-PCR can be positive for several weeks in patient stool and even detectable in sewage works, with viable virus isolated in only one reported case. In the overwhelming majority (bar one case), live virus was not isolated.59–61
These data on the likely infectious nature of stool provide significant reassurance but could not support the complete abrogation of all PPE. It is reasonable, however, that lower GI procedures are treated as lower risk in terms of transmissibility than upper GI (though both are still aerosol-generating). Thus, if patients have been asymptomatic for both respiratory and GI symptoms for 14 days prior to endoscopy and have a negative nasopharyngeal swab prior to their appointment, this could allow the use of low-risk (level 1) PPE62 and less stringent IPC strategies for lower GI endoscopy, facilitating higher throughput and aiding recovery. It should be noted that low-risk PPE in previous descriptions involves the use of long-sleeved gowns.62
Room cleaning is an essential part of IPC strategy. High-level strategies are already implemented after an endoscopy has been performed, for instance, in patients with antibiotic-resistant infection. All units will have such strategies in place. This will clearly delay room turnover and highlights the need for a stratified approach. To reiterate, if patients are proven COVID-19-negative prior to attendance, there is no need for such strict policies to remain in place, and the COVID-minimised workstream can be fully realised. If stricter PPE policies remain in place, with the use of high-risk (level 2) PPE and high-level IPC strategies, it is reasonable to expect that units would only achieve a maximum of 35% of prepandemic capacity.17 We estimate that a stratified strategy could reach 75% capacity or more, but this remains to be tested.
Scope: staffing units
It is crucially important that units protect their staff from unacceptable exposure to COVID-19 and is a core responsibility of any employer. In addition, staff absence through infection may significantly impact endoscopic activity but also presents a risk to patients and other staff if staff members become infected and attend work. Staff will, therefore, also require enhanced screening to maintain COVID-minimised units. For example, online or self-reported prework symptoms and fever-free confirmation (as for patients prior to attendance) have been described at one major US hospital system.63 A further option is to divide staff into COVID-minimised and ‘hot’ teams, with no interaction or cross-working between corresponding areas without negative swabs in between. Widespread systematic testing of hospital staff may facilitate this further but is likely to be subject to local infection control policies.
While the term ‘cold’, ‘clean’ or ‘COVID-free’ unit is appealing and may help both staff and public engagement with necessary procedures, it is critically important to remember that these are COVID-minimised endoscopy units and are not entirely risk-free. The degree of risk minimisation will vary, depending on the ability of units to effect screening procedures and alter their physical patient pathways and standard operating procedures.
‘Survey’: postprocedure surveillance
Inherent in the maintenance of a COVID-minimised facility will be surveillance of patients after their procedure for the development of symptoms. In line with other recommendations,3 5 35 62 we recommend telephone follow-up of patients (online tracking tools should make this easier in the long term) at 7 and 14 days after endoscopy to check for development of symptoms. The expected incidence of this phenomenon is reportedly low64 but requires confirmation in other healthcare systems and should be part of routine vigilance. If cases emerge, a detailed case study should be initiated to determine the potential source (and contact tracing may be appropriate). This will also quality-assure the success of the proposed measures and inform planning for any future outbreaks.
Conclusion
It is imperative that measures are developed to allow restoration of endoscopy capacity at scale. We present a strategy for a risk-stratified return to endoscopic activity based on the current available science and experience worldwide. Systematic testing of both patients and staff, with rapid turnaround of results, scheduling of patients in pathways appropriate to the type of endoscopy and their COVID-19 status, as well as follow-up after the procedure, will allow resumption of significant levels of activity. Without these measures, particularly if units adhere to peak-pandemic levels of infection control, endoscopic activity will remain severely curtailed for extended periods and will likely not reach more than 35% of pre-existing capacity.17 With a range of measures, including the early establishment of COVID-minimised pathways or sites, as well as robust management of demand, endoscopy systems can be restored.
These principles could be applied to other medical specialities where invasive diagnostic procedures are performed.
In accordance with WHO, national and international society guidelines, inherent to the establishment of any new pandemic-response pathways, is a systematic programme of monitoring for effectiveness and safety. This includes not only screening strategies such as the one detailed herein, but also an assessment of harm due to delayed procedures is also vital. This is an essential part of preparedness and ensures our current practice is optimised and will facilitate the safe, effective and efficient services that our patients and stakeholders will expect and need.
Acknowledgments
The authors thank the members of the British Society of Gastroenterology (BSG) Endoscopy Committee, the BSG Endoscopy Quality Improvement Programme and the UK Inflammatory Bowel Disease COVID-19 working group.
References
Footnotes
Twitter @IBDdoc
Contributors All authors contributed to the preparation of this manuscript.
Funding JE was funded by the National Institute for Health Research Oxford Biomedical Research Centre.
Competing interests JE served on the clinical advisory board for Lumendi and Boston Scientific and the clinical advisory board and ownership for Satisfai Health; and received speaker fees from Falk. CJR received grant funding from ARC Medical, Norgine Pharmaceuticals UK, Olympus Medical UK, 3D Matrix and was an expert witness for ARC Medical. BH received grant funding from Olympus Medical UK, Fujifilm Europe, Takeda Pharmaceuticals UK and AbbVie UK, and served on the clinical advisory board and ownership of Ampersand Health, Surgease Medical Ltd.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.