Article Text

Statistics from Altmetric.com
Introduction
Climate change has been described as ‘the biggest global health threat of the 21st century’.1 Medical professionals have a vital role in mitigating the impact of healthcare systems on the environment and protecting vulnerable people through the development of sustainable clinical practices.
We have previously written about how gastroenterologists must act now to change our endoscopy practice and make it more aligned with core principles of environmentally sustainable healthcare. But it is clear there is a significant lack of evidence to accurately define the scope of the environmental impact of gastroenterology services, or models of best practice to shape policy and move the field in a new direction.
This article aims to provide a framework for us to design and implement quality improvement projects (QIPs) in gastroenterology as a strategy to deliver a more sustainable future in line with the National Health Service (NHS) Net Zero targets.2 Mortimer et al have described the key principles required,3 4 and we aim to apply these to a gastroenterology context and specifically endoscopy services.
The triple bottom line
The value of a healthcare intervention relates to the outcomes delivered against its cost, and the benchmark for cost-effectiveness set by the National Institute for Health and Care Excellence is £20–30 000 per quality-adjusted life year gained.5 However, economists interested in sustainability recognise that costs also need to recognise the social and environmental impact of what is consumed: the so-called ‘triple bottom line’.6 Value can thus be presented using this schematic formula as described by Mortimer et al 3:
Value=outcomes for patients and populations/environmental+social+financial impacts.
Considered in this way, every healthcare intervention has not only financial implications, but also a social cost on the patient and their family/carers, and environmental implications from resource use and carbon footprint, against which the clinical benefit needs to be weighed.
Incorporating these considerations into guidelines, policies and commissioning will be complex and require both strategic vision and an evidence base. One approach could be to use grass-roots quality improvement programmes targeted to maximise the value of the interventions delivered in our services, which may in time inform higher level decisions.
Establishing aims
Ultimately, our aim is to maximise the value of our healthcare services, optimising individual and population health outcomes while minimising the environmental, social and financial cost (the triple bottom line). Moving environmental and social impact up the agenda of service improvement schemes alongside financial considerations is vital not only to realign our values to a sustainable way of working but also to raise staff morale and motivate them in designing a sustainable workplace. A recent survey conducted by the NHS Sustainable Development Unit showed that 98% of NHS staff believe that health and care systems should work in ways to support the environment.7 For a busy team with many additional time commitments, placing improvement work within a vision of sustainability will help the team engage with the project.
Understanding what you do: process mapping
The first step is to identify the aspects of our practice on which to focus.
Consider endoscopy: each investigation requires numerous steps from the decision to request through to actioning the result (figure 1). Process mapping can be used to identify which step(s) can be targeted to maximise value. For example, this may identify a longstanding problem with a large volume of low-yield procedures, which may either be clinically unnecessary or may have lower carbon alternatives. Alternatively, there may be inefficiencies in the process of organising and following up the procedure that are wasteful in resource use, such as travel time for face-to-face appointments to discuss results that could be done remotely.
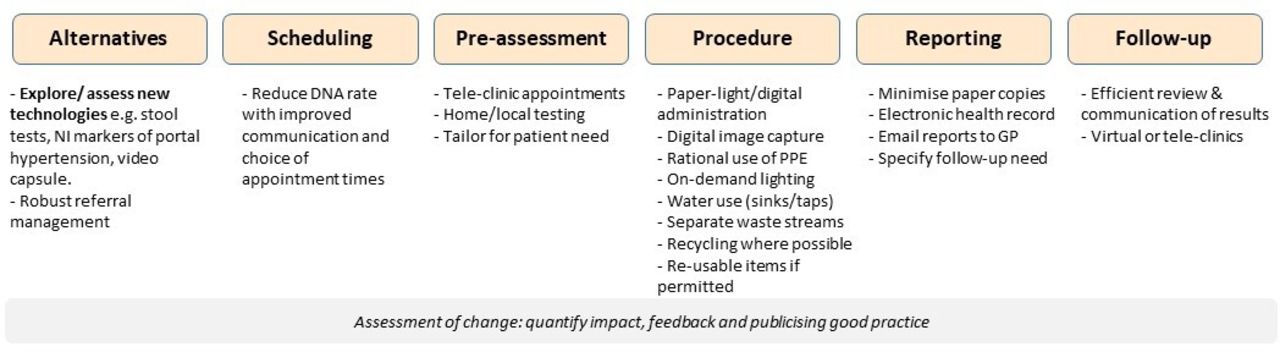
Process mapping for endoscopy. More sustainable alternatives could be considered at each step and used as a focus for the development of a quality improvement project. DNA, did not attend; GP, general practitioner; NI, non-invasive; PPE, personal protective equipment.
Broader research into ‘carbon hot spots’ in healthcare has identified building energy inefficiencies and medical equipment as the main sources of carbon use in acute hospitals. Therefore, reducing procedure numbers is likely to have the biggest impact on the environmental cost.2 8 However, we must also optimise the way we use resources in the procedures we should continue to deliver. At each step there are opportunities to consider sustainable alternatives (figure 1).
Designing ‘green endoscopy’ quality improvement plans
A helpful framework for sustainable healthcare systems to inform QIP design has been proposed by the Centre for Sustainable Healthcare, incorporating four key principles: (1) prevention; (2) patient empowerment; (3) lean systems and pathways; (4) preferential use of technologies with a lower environmental impact.3
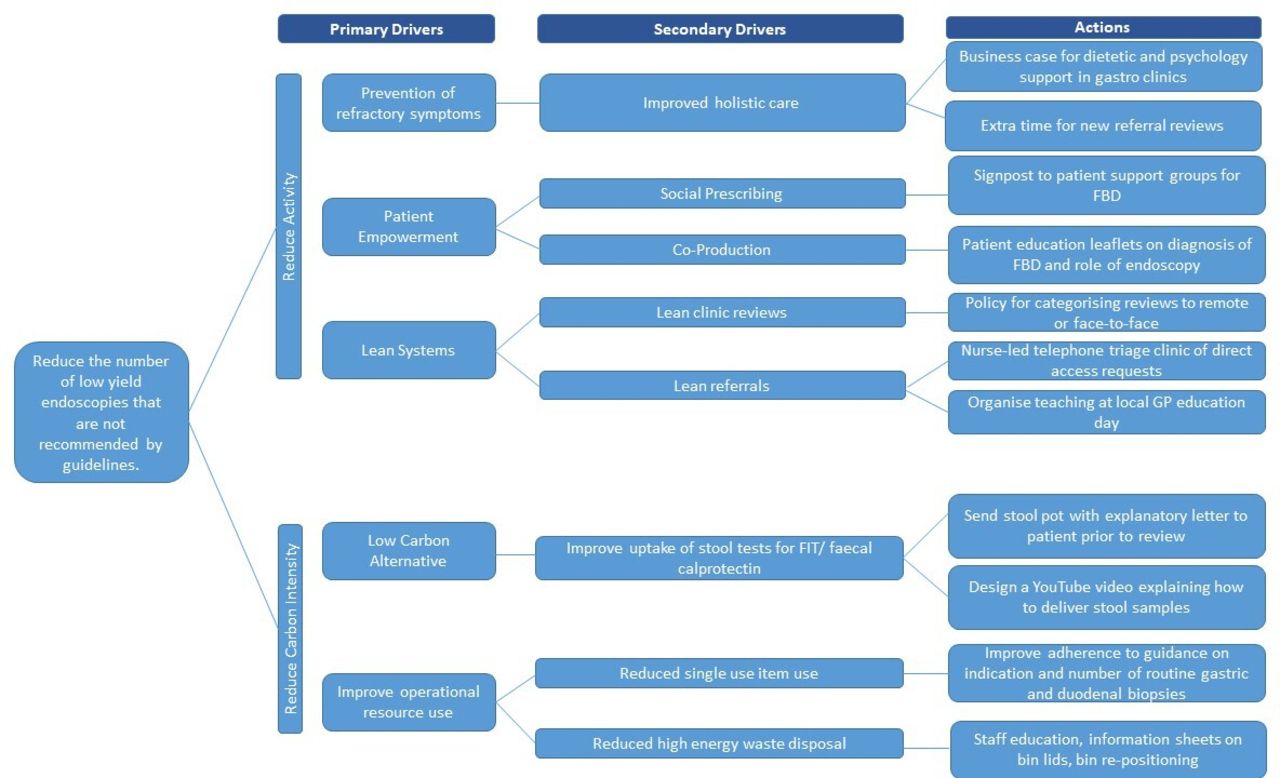
These core principles can be incorporated into a ‘driver diagram’ to identify primary and secondary drivers of the desired change and potential actions for improvement. Figure 2 is an example of this; a QIP may only focus on one part, but it illustrates how action points may be generated. For example, a unit may audit and find patient uptake of stool tests for calprotectin to be low, increasing the number of colonoscopies requested for patients with a diagnosis of irritable bowel syndrome. This may prompt the development of novel educational materials to help improve patient acceptability and uptake. Alternatively, there may be inappropriate referrals to gastroscopy (eg, low-risk dyspepsia or normocytic anaemia). A dedicated nurse-led telephone triage and vetting clinic may divert patients to more appropriate investigation and management.
{kind=link}
{kind=link}
Driver diagram for a ‘green endoscopy’ QIP. This worked example includes more than could be addressed in a single QIP, but illustrates how action points may be generated through considering the drivers for the desired change, based on the core principles of sustainable healthcare.3 FBD, functional bowel disease; FIT, faecal immunochemical test; GP, general practitioner; QIP, quality improvement project.
For the procedures that are performed, simple measures could be put in place to improve waste segregation. It is a common problem for waste that may otherwise be recycled (lowest carbon emissions) being incorrectly placed in bins destined for high-temperature incineration (highest carbon emissions). Simple steps such as optimising bin positioning in endoscopy rooms, clearly labelling bin lids with what should be placed in them or a staff education session led by the trust green champion could have significant impact (figure 2).
Measuring the impact and value of the QIP
All hospitals will be interested in projects aimed at saving money, and a focus on efficient systems and low carbon alternatives will often lead to reduced financial costs. But as discussed above, this is just one aspect of the true cost of our service; we also want to assess the environmental impact of what we do.
Consider the above example, where a service identifies a group of endoscopic procedures that could be reduced through more effective vetting and use of stool biomarkers. The calculation of the carbon footprint of an endoscopic procedure is complex, and although some early work has been done in parallel fields such as urology,9 this is an unmet research need in gastroenterology. However, a secondary impact is reduced patient travel. Part of the outcome measure could be calculating the car journeys saved and the resulting reduction in carbon emissions (eg, https://calculator.carbonfootprint.com/calculator.aspx?tab=4). Combining this with a patient survey on time saved and level of inconvenience will help to quantify some of the social impact of the intervention.
A project on waste disposal will give an opportunity to start working more closely with the estates team. Previous studies have quantified the carbon emissions arising from different forms of waste disposal, and these could be used to quantify the impact of improved waste segregation and reduce forms of unnecessary waste in the unit.10
Dealing with the COVID-19 backlog: an opportunity to implement sustainable practice
Data from the National Endoscopy Database indicate that total endoscopy activity fell rapidly to 5% of normal levels during the peak phase of the COVID-19 epidemic in the UK.11 Analysis from the first wave of COVID-19 predicted a backlog of almost half a million endoscopic procedures by January 2021. Increasing capacity to 130% would take until June 2022 to eliminate the backlog.12
Addressing this problem through upscaling prior practice will exacerbate what the WHO estimates is a 40% month on month increase in personal protective equipment (PPE) production during the pandemic.13 Moreover, all endoscopy activities carry significant infection-control risk as aerosol-generating procedures.
This represents an excellent opportunity to expedite the implementation of waste-reducing practices linked to robust senior vetting procedures. Travel to hospital should be minimised, recycled paper and plastic products used in preference and sustainable practice in PPE implemented (which should be a sector-wide strategy).14
Embedding change within unit accreditation
In the UK, endoscopy unit quality is developed and maintained through the Joint Advisory Group (JAG) accreditation process. A new section on ‘green endoscopy’ has been added to the updated Global Rating Scale, currently out for stakeholder review. This is a welcome and crucial step in the right direction to formally embed sustainable principles into our practice.
Opportunities for research
There are many unmet needs for future research in this field, including understanding the true carbon footprint of endoscopy procedures, waste generation and optimal streams of disposal, and implementation of low carbon alternatives. A network of ‘green champions’ must be implemented to help generate, disseminate and implement best practice in this regard.
In the context of quality improvement, sustainability is commonly associated with an ability to maintain and continually build on improvements made. However, we now need to challenge and broaden this definition such that sustainability refers to the capacity of a health service to deliver healthcare over time, with consideration to future generations.3
Conclusions
There is growing awareness among the gastroenterology community that our services need to develop to align with sustainable healthcare values and help address the climate crisis. Well-designed quality improvement initiatives can begin to move us in the right direction, and we hope this will be augmented by emerging research in this vital field.
Ethics statements
Patient consent for publication
Footnotes
Twitter @jamesbmaurice, @andrewrochford, @SarahTom123, @anjan_dhar6, @IBDdoc
Collaborators We wish to thank the other members of the 'Green Endoscopy' group for their contribution to the ideas resulting in the development of this article: Keith Siau, William Stableforth, Emma Wesley, Swapna Gayam, Nitin Ahuja, Sandeep Sidhi and Andrew Veitch.
Contributors JBM conceived and wrote the manuscript and designed figure 2. BH assisted in manuscript conception, designed figure 1, provided important intellectual content and critically reviewed the manuscript. AR wrote the section on dealing with the COVID-19 backlog and critically reviewed the manuscript for important intellectual content. SM, SS and AD provided important intellectual content and critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JBM reports non-financial support from Norgine, personal fees and non-financial support from Intercept Pharma outside the submitted work. SS reports research grants from Takeda, Pfizer, Tillotts Pharma and AMGEN; speaker fees and or advisory board honoraria fees from Pfizer, Takeda, Tillotts, Pharmacocosmos, Jaansen, AMGEN and Abbvie outside the submitted work. BH reports grants from Fujifilm Europe, other from Ampersand Health, other from Surgease Medical outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.