Article Text

Statistics from Altmetric.com
Liver transplantation (LT) is a life-saving treatment for patients with end-stage chronic liver disease. Given the negative impact of distance from transplant centre on patient outcomes,1 2 King’s College Hospital (KCH) developed a network of satellite liver transplant centres (SLTCs) in Plymouth and Belfast to optimise access to LT.3 These centres deliver transplant assessment and comparable post-LT care to conventional LT centres.4 However, patients are still required to complete their assessments at KCH prior to listing.
The COVID-19 pandemic has caused unprecedented strain on health services globally. The UK LT programme was affected with transplantation and assessment occurring only in patients with urgent need.5 However, patients at SLTCs were also subject to travel restrictions which further disadvantaged them compared with local patients. A virtual transplant assessment (VTA) pathway was developed to allow SLTCs to assess their patients for LT locally and to discuss listing without attendance at KCH. Here, we describe our first experiences with this novel pathway.
We retrospectively included all patients from both SLTCs who completed an LT assessment between April 2020 and April 2021. The decision for a VTA was made by consensus decision from the multidisciplinary teams at the relevant SLTC and KCH (online supplemental figure 1). While there were no strict criteria defining selection of assessment pathways, if there were significant concerns regarding a patient’s transplant candidacy they underwent a face-to-face assessment (FTFA).
Supplemental material
Patients’ clinical notes were interrogated for demographic data, clinical data and laboratory data from time of assessment. Outcomes including time from listing to transplantation and short-term post-LT outcomes were also evaluated. Patients undergoing FTFA were directly compared with those undergoing VTA. A p value of <0.05 was considered statistically significant (*). All analyses were performed using Prism V.9.1.2 (GraphPad, San Diego, California, USA).
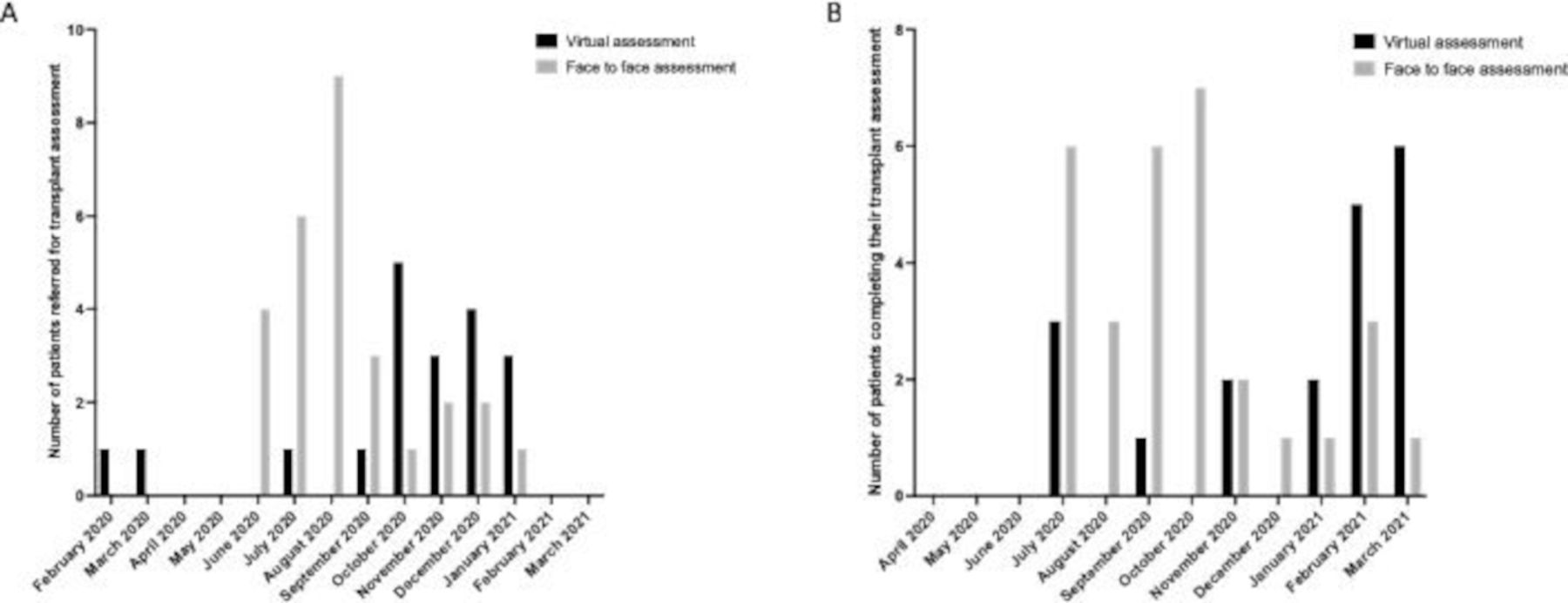
Forty-nine patients from SLTCs underwent transplant assessment during this period (19 VTAs and 30 FTFAs). Figure 1A demonstrates when patients were referred for LT assessment and figure 1B demonstrates when patients had completed their LT assessment. Of note, the VTA pathway was used for two patients referred prior to the pandemic. It also shows the VTA pathway being increasingly used after September 2020 (figure 1A), and this overtook the FTFA pathway in 2021 as the primary assessment pathway for patients referred from SLTCs. Patients assessed via VTA had an increased time from referral to completion of their assessment (p=0.01*) (online supplemental table 1). However, patients referred in 2021 to the VTA pathway had a shorter time to completion of their assessment than those referred in 2020 (n=3, median 38 days (IQR 25–55), versus n=16, median 83 days (IQR 48–130.3)). This likely reflects that the pathway was used to clear the initial backlog of referrals as well as the initial challenges in establishing a new pathway. The VTA pathway remained functional through the second wave of COVID-19, whereas the FTFA pathway did not.
{kind=link}
Time of referral and completion of LT assessments in patients from SLTC. (A) Number of patients referred per month for patients completing LT assessments from SLTCs between April 2020 and April 2021. (B) Number of patients completing assessments per month from SLTCs between April 2020 and April 2021. LT, Liver transplantation; SLTC, satellite liver transplant centre.
Online supplemental table 1 demonstrates the characteristics of each patient cohort. While there was a trend for patients in the VTA cohort to be younger, no significant differences were demonstrated between the two cohorts for demographic or clinical variables, prognostic scores or likelihood of listing for LT. However, we must acknowledge that our results are preliminary, and differences between cohorts may become apparent as we assess more patients. We anticipate that FTFA will be reserved for patients with more complex liver disease and comorbidities.
Of the patients listed for transplant, no patients were delisted following listing in the VTA cohort. Three patients were delisted in the FTFA cohort. Six patients from the VTA cohort and 11 patients from the FTFA pathway were transplanted during the study. Survival analysis demonstrated no difference in time from listing to transplantation between each cohort (p=0.25). No patients in the VTA pathway had a surgical complication; median intensive care and KCH inpatient lengths of stay were 1.5 and 11.0 days respectively. These data are reassuring for the safety of the VTA pathway, although longer-term follow-up data are required to evaluate this pathway. Furthermore, patient and healthcare professional satisfaction needs to be evaluated.
We describe the first UK experience of a VTA pathway in LT. While our experience is preliminary, we demonstrate that this pathway is feasible and may increase access to transplantation for patients and address a well-documented healthcare inequity.1 2
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @OTavabie
Contributors All authors contributed to conceptualisation and design. Data collection was performed by AP, FB, KR and WL. Data analysis and interpretation were performed by ODT. The manuscript was drafted by AP, FB and VRA. All authors made critical revisions and approved the final version of the manuscript
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.