Article Text

Abstract
Background—Medium chain C8–C10 triglycerides (MCTs) improve fat absorption in short bowel patients. Effects on overall energy absorption remain unknown.
Aims—To determine whether MCTs and medium chain fatty acids (MCFAs) are absorbed in the colon like the short chain fatty acids (SCFAs) or are lost in faeces similarly to long chain fatty acids (LCFAs).
Methods—Nine small bowel resected patients without and 10 with a colon in continuity excreted 2–6 MJ/day and were randomised and crossed over between two high fat diets (10 MJ/day, 50% as fat), based on either long chain triglycerides (LCT) alone or equal quantities of LCT and MCT.
Results—Patients with a colon absorbed C8–C10 fatty acids considerably better than patients without a colon at similar and extreme levels of LCFA malabsorption; the colonic impact on absorption of C14–18 fatty acids was negligible. MCT redoubled fat (MCT+LCT) absorption from 23% to 58% in patients with a colon, and increased overall bomb calorimetric energy absorption from 46% to 58%. The increase in fat absorption from 37% to 46% in patients without a colon did not improve overall energy absorption because malabsorption of carbohydrate and protein increased.
Conclusion—In small bowel resected patients, the colon seems to serve as a digestive organ for medium chain fat, probably absorbed as MCFAs, perhaps because like the SCFAs, they are water soluble. Only patients with a colon gained from MCT treatment.
- absorption
- medium chain fatty acid
- colon
- short bowel
Statistics from Altmetric.com
Carbohydrate and protein that escape absorption in the small bowel are metabolised by the colonic bacteria to short chain fatty acids (SCFAs), which are readily absorbed in the large bowel. This type of digestion is well known from the rumen and large bowels of plant eating animals, and it represents a means of salvaging energy in patients with short bowel and preserved colonic function, having been shown to reduce faecal energy excretion by 2–4 MJ/day.1-3
Medium chain triglyceride (MCT) has been applied in therapy when assimilation of dietary long chain triglyceride (LCT) is diminished. A reduction in steatorrhoea has been taken as the clinical argument for this treatment, and emphasis has been placed on the more rapid absorption of MCT in the small bowel.4 ,5 The human colon is not usually considered as a site of fat absorption, although studies have indicated that colonic absorption of the medium chain fatty acids (MCFAs) C8:0 and C10:0 takes place in dog6 and rat.7 ,8 The increase in octanoic acid in peripheral blood after rectal installation in patients with cirrhosis,9 and the rectal absorption of octanoic acid from dialysis bags10 implies that MCFAs are absorbed in the human rectum.
The awareness of SCFA absorption in the large bowel prompted us to investigate whether the favourable absorption also holds for MCFAs, and to what extent preserved colonic function exerted an influence on the efficacy of MCT treatment in patients with small bowel resection.
Material and methods
PATIENTS AND STUDY DESIGN
Patients with small bowel resection and a faecal loss of energy between 2 and 6 MJ/day on their habitual diet were considered as study participants. Patients with recent surgery (within one year) and inflammatory bowel disease with signs of active inflammation were not included. Two high fat diets (LCT and LCT+MCT) were designed from food tables to provide the same energy equivalent of 20:24:56% carbohydrate:protein:fat and total energy content as obtained from dietary records. Duplicate diets were prepared; one for analysis.
The LCT diet was based on ordinary dietary fat, whereas half of the LCT (weight ratio) was replaced by MCT in the LCT+MCT diet by the use of MCT containing margarine (Van den Bergh Foods, Rotterdam, The Netherlands), MCT oil, Triglydal (Laboratorie Sodietal, France), and an MCT oil emulsion, Liquigen (Nutricia/Scientific Hospital Supplies, Liverpool, UK). Patients were hospitalised for nine days and diets were given for four days each in a randomised crossover design separated by one day. The last three of the four days served as test periods. Patients were allowed an unrestricted but recorded intake of no energy beverages; medications and parenteral supplements were kept constant. Stools were collected on ice and immediately frozen at −20°C. Analysis was done on homogenised and freeze dried aliquots of 24 hour pooled dietary and faecal samples.
Twenty four patients were studied, of whom five were excluded: three felt distaste for and were unable to eat the high fat diets as prescribed, while two experienced abdominal discomfort and chose not to continue. A total of 19 therefore completed the study (table 1). Six patients had a jejunostomy (less than 200 cm jejunum remnant), and three had an ileostomy with ileal resections of 50, 50, and 85 cm, respectively. These nine patients comprised six women and three men (aged 28–74 years); indications for jejunostomy or ileostomy were Crohn’s disease (n=6), colectomy for ulcerative colitis and small bowel infarction (n=1) or a removed Koch’s reservoir (n=1), and complications after surgery (n=1). Mean residual small intestine was 203 cm (range 125–300 cm). Four received parenteral nutrition or fluids (0.9–4.5 l/day; 0–3.4 MJ/day). Mean time from last resection was 9.8 years (range 1.1–18.0 years). Ten patients had small bowel resections with a colon in continuity (four women and six men, aged 20–78 years), due to Crohn’s disease (n=6), infarctions (n=2), volvulus (n=1), or complications after a cholecystectomy (n=1). Three patients had a full colon with preserved ileocaecal valve (and 10 cm of remnant ileum), three had an ileocecal resection (two with a total ileum resection and one with resection of 100 cm), and four had a right sided hemicolectomy (two with jejunoascendo anastomosis and two with ileum resections of 100 and 110 cm, respectively). None of the 10 had a colostomy. Mean residual small intestine was 143 cm (range 50–250 cm). Two received parenteral nutrition (1.9–2.6 l/day; 6.4 MJ/day). Mean time from the last resection was 5.3 years (range 1.4–11.9 years).
Patient characteristics
ANALYSIS
Dietary and faecal energy were determined by bomb calorimetry in an IKA adiabatic calorimeter, model C 4000 A (IKA-Analysentechnik, Heitersheim, Germany). The energy conversion factors were those of Atwater et al confirmed by Southgate11: 0.0176 MJ/g and 0.0236 MJ/g for carbohydrate and protein, respectively. Heats of combustion (MJ/mol) of fatty acids were −ΔHc = 0.653n − 0.166d − 0.421, where n was number of carbon atoms, d the number of double bonds.12 Absorption of LCT, MCT, and total fat was based on the assumption that fat was ingested as the triglyceride, but excreted as free fatty acids—that is, 1 mol of glycerol (1.66 MJ/mol) was added to every 3 mol of dietary fatty acids. Nitrogen was determined by the technique of Kjeldahl,13 and carbohydrates by acid hydrolysis and colorimetry at 530 nm as described by Englyst and Cummings.14
Fatty acids were determined by combined gas liquid chromatography (GLC) and mass spectrometry (MS). Internal standards were C9:0, C13:0, and C17:0. Half a gram of homogenised faeces or diet was added to 1 ml of KOH 33% and 4 ml of ethanol:amyl alcohol (94:4) in tubes equipped with Teflon lined screw caps and incubated in a boiling water bath for 30 minutes. Ethanol was evaporated and 1.7 ml of 6 mol/l HCl and 5 ml of hexane were added to cooled tubes and shaken vigorously before centrifugation for five minutes at 600 g. A 500 μl aliquot of the hexane phase was transferred and evaporated under nitrogen before methylation with 1 ml of 14% boron fluoride in methanol (BF3) in a boiling water bath for two minutes.15 After cooling, 2 ml of hexane and 1 ml of water were added before the hexane phase was transferred to sealed vials and fatty acid methyl esters were quantified by GLC-MS on a Hewlett Packard 5890 chromatograph with a 25 m fused silica capillary column (0.32 mm internal diameter, BPX70, Microlab, Aarhus, Denmark) equipped with a Hewlett Packard 5971A mass spectrometer. Peak areas of C8:0, C10:0, C12:0, C14:0, C16:0, C16:1, C18:0, C18:1, C18:2, C18:3, and C20:0 fatty acids were calculated from total ion chromatograms. Intestinal bacteria are able to convert part of unsaturated LCFAs to the isomer and the hydroxy LCFAs at the position of the double bond; for example, oleic acid, C18:1, may convert to 10-hydroxystearic acid, 10-OH-C18:0.16-18 Therefore, faecal excretions used for calculation of absorption of unsaturated LCFAs were the sum of unsaturated fatty acids added to their corresponding isomers and hydroxy acids. The carrier gas was helium. Oven temperatures were 60°C for two minutes, followed by an increase of 4°C per minute until 250°C which was maintained for 60 minutes.
STATISTICS
Results are expressed as means (SD) and tested for statistical significance with Student’s t test for paired and unpaired data and one way analysis of variance (ANOVA). All pairwise multiple comparisons, Student-Newman-Kreuls method, was used as the post hoc test. A value of p<0.05 was considered significant.
ETHICS
Procedures followed were in accordance with the ethical standards of the 1975 Helsinki Declaration, as revised in 1983, and the study was approved by the Ethics Committee for Medical Research in Copenhagen, Denmark.
Results
Table 1 gives baseline patient characteristics.
ABSORPTION OF FATTY ACIDS WITH DIFFERENT CHAIN LENGTHS
Figure 1 shows the absorption of individual fatty acids during the LCT and LCT+MCT periods. Figure 2 illustrates that the absorption in percentage of intake during the LCT+MCT period was inversely related to chain length in both groups of patients. The percentage of absorbed LCFAs was not significantly different between patients with (22 (24)%) and without (27 (24)%, p=0.69) a large bowel in contrast to the absorption of C8:0 (no colon 63 (25)% versus colon 96 (3)%; p=0.0007) and C10:0 (no colon 57 (28)% versus colon 87 (6)%; p=0.004). This was because faecal excretion of C8:0 in patients with preserved colonic function on the LCT+MCT diet was only 3% of intake, 10 times lower than C8:0 excretion in patients with no colon (p=0.0004); furthermore, excretion of C10:0 was only 12% of intake in patients with a colon, four times lower compared with patients without a colon (p=0.016).
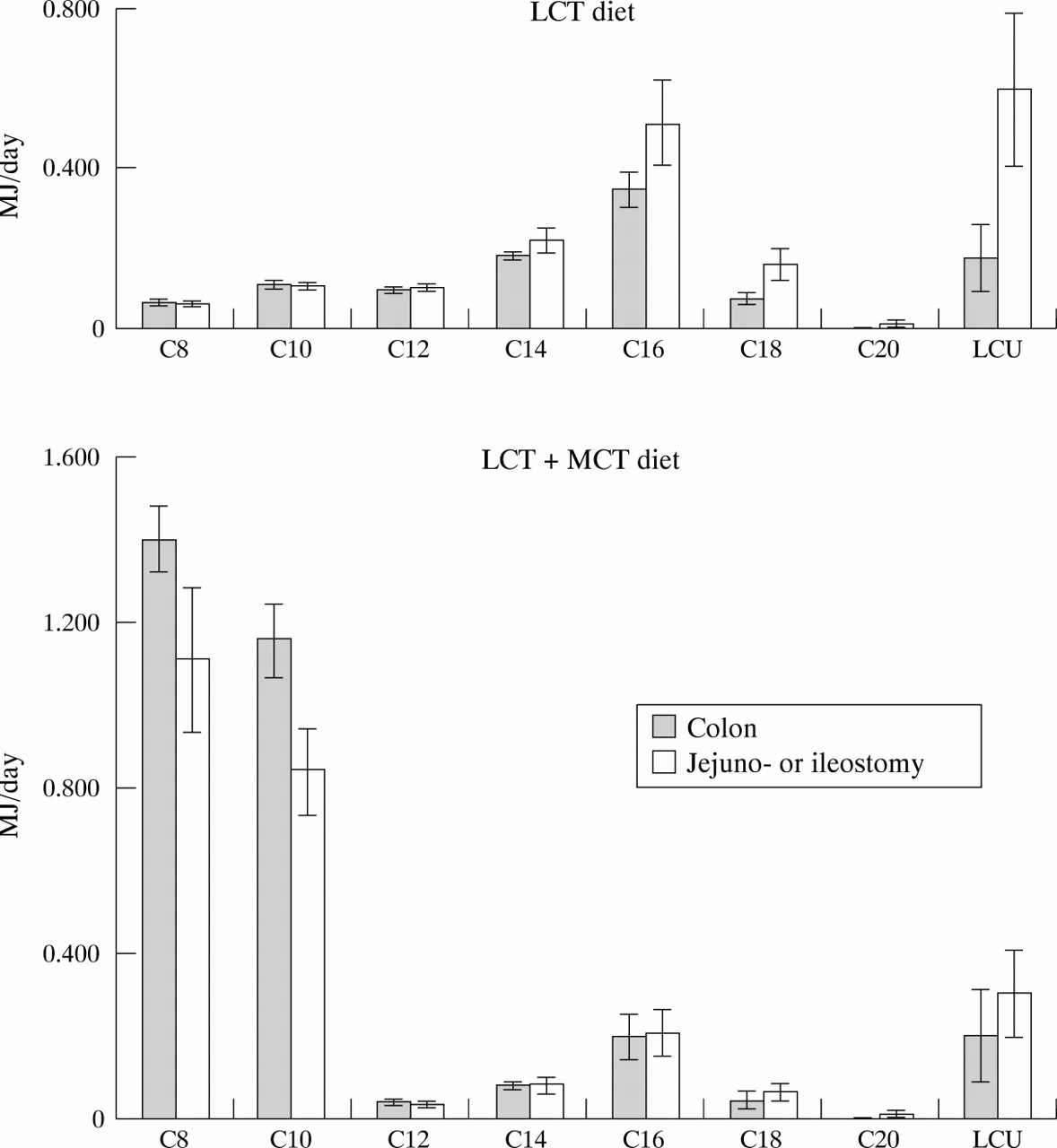
Absolute absorption of saturated fatty acids C8, C10, C12, C14, C16, C18, C20, and long chain unsaturated fatty acids (LCU, includes C16:1, C18:1, C18:2) in patients with small bowel resection with and without a preserved colon during the LCT diet and LCT+MCT diet. Results are given as mean (SEM).

Relative absorption of saturated fatty acids C8, C10, C12, C14, C16, C18, C20, and long chain unsaturated fatty acids (LCU, includes C16:1, C18:1, C18:2) in patients with small bowel resection with and without a preserved colon during the LCT+MCT diet. Results are given as mean (SEM).
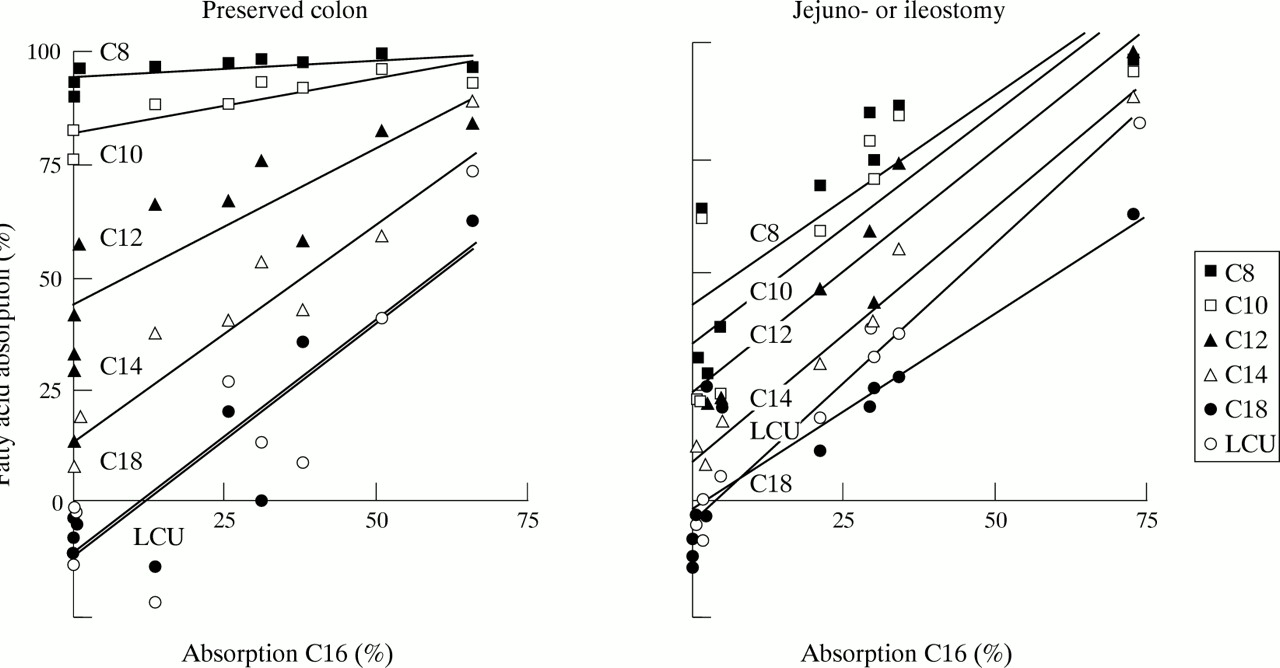
ABSORPTION OF INDIVIDUAL FATTY ACIDS AS A FUNCTION OF C16:0 ABSORPTION
Dietary C16–C18 LCFAs were completely (98–100%) malabsorbed in three patients with a preserved full colon and ileocaecal valve and in one patient with half a colon in continuity. None of these patients had more than 10 cm of ileal remnant. This indicates that LCFAs with a length of 16 or more carbon atoms are not absorbed in the colon—that is, absorption reflects small bowel absorption only. Due to its dietary abundance, in fig 3, C16:0 was chosen as a best measure of the isolated small bowel absorption of LCT, against which the absorption of other fatty acids was shown for individual patients on the LCT+MCT diet. The line of absorption for fatty acids that were better absorbed than C16:0 would be located above the diagonal, X=Y in fig 3. This was seen for the shorter chained fatty acids in both groups of patients—that is, at a given low level of C16:0 absorption, C8:0–C14:0 were absorbed better in a chain length dependent pattern. If the preservation of a colon improves absorption of C8:0–C14:0 further, the line of absorption in patients with a colon would appear above the line of absorption in patients without a colon, which was clearly the case for the MCFAs. The absorption of C8:0 was almost complete (more than 90%) at any level of C16:0 absorption in patients with a functional colon—that is, independent of the level of preserved small bowel absorption of LCT. Intercepts for the lines of absorption of C8:0 at no absorption (0%) of C16:0 were 94 (1)% and 43 (7)% for patients with and without a colon, respectively (p<0.001), and slopes were 0.08 (0.03) and 0.91 (0.22), respectively (p<0.01). Similarly, the absorption of C10:0 was considerably better in patients with a colon, while the colonic influence was small on C12:0 absorption and not noticeable on the absorption of C14:0, C18:0, and the unsaturated LCFAs (fig3).
{kind=link}
{kind=link}
{kind=link}
Relative absorption of saturated fatty acids C8, C10, C12, C14, C18, and long chain unsaturated fatty acids (LCU, includes C16:1, C18:1, C18:2) in relation to absorption of C16 in patients with small bowel resection with and without a preserved colon during the LCT+MCT diet.
ABSORPTION OF CARBOHYDRATE, PROTEIN, FAT, AND ENERGY
Table 2 shows results of the analysis of dietary intake, faecal excretion, absolute and relative absorption of carbohydrate, protein, fat, and energy. Total energy absorption did not change in patients with no colon, when they changed from the LCT to the LCT+MCT diet, neither when total energy was calculated from the sum of carbohydrate, protein, and fat (5.407 (1.478) versus 5.612 (1.837) MJ/day, p=0.63; equal to 53 (18)% versus 51 (20)% of dietary intake, p=0.56), nor when measured by bomb calorimetry (4.819 (1.912) versus 5.212 (1.556) MJ/day, p=0.42; equal to 47 (23)% versus 49 (19)% of dietary intake, p=0.63). MCT did, however, improve overall fat absorption (MCT+LCT) by 0.899 (0.748) MJ/day (p=0.001) from 37 (26)% to 46 (24)% of dietary fat intake (p=0.05), but this change for the better was counterbalanced by a 0.252 (0.279) MJ/day decrease in absorption of carbohydrate (p=0.03) and a 0.443 (0.366) MJ/day decrease in absorption of protein (p=0.01).
Diet and faeces energy content, and absolute and relative absorption
MCT increased fat absorption by 2.079 (0.890) MJ/day from 1.042 (0.469) to 3.121 (0.779) MJ/day (p<0.001) in patients with colon in continuity, which was equal to an increase from 23 (10)% to 58 (15)% of dietary intake of fat (p<0.001, table 2)—that is, fat absorption was improved substantially more than in patients without a colon, and no effect on the absorption of carbohydrate and protein was encountered. Hence the beneficial effect on fat absorption was passed on to an overall improvement in energy absorption of 1.774 (1.559) MJ/day (p<0.01), corresponding to an increase from 51 (7)% to 64 (13)% of total dietary energy intake (p=0.01), when measured as the sum of the analyses of carbohydrate, protein, and fat. Bomb calorimetry revealed a similar 1.308 (1.346) MJ/day (p=0.01) increase in energy absorption, which was an improvement in energy absorption from 46 (9)% to 58 (11)% of dietary intake (p=0.02, table 2).
Stoma effluents tended to increase in patients with no colon when they were changed from the LCT diet (2177 (1455) g/day) to the LCT+MCT diet (2729 (1543) g/day; p=0.07), in contrast to patients with a colon, who had equal faecal volumes during the LCT diet (981 (379) g/day) and the LCT+MCT diet (1114 (622) g/day; p=0.32).
The amounts of the individual MCFAs and LCFAs (not shown) and of total fat (table 2) administered in either the LCT or the LCT+MCT diets to the two groups of patients were not significantly different. However, the total content of energy in the LCT diet was approximately 0.900 MJ/day lower than in the LCT+MCT diet, because food table analysis overestimated the content of LCT compared with laboratory analyses. Deviations between food table and laboratory analysis of MCT, carbohydrate, and protein were negligible. Dietary energy calculated as the sum of laboratory analyses of carbohydrate, protein, and fat matched bomb calorimetry measurements completely (laboratory:bomb ratio, 99 (6)%). Dietary energy ratios between MCFAs, unsaturated LCFAs, and saturated LCFAs were 4%:41%:55% in the LCT diet and 51%:25%:24% in the LCT+MCT diet. Dietary MCFAs were C8:0 (52%, octanoic acid) and C10:0 (48%, decanoic acid). C16:0 (palmitic acid), C18:0 (stearic acid), and C18:1 (oleic acid) provided approximately 75% of LCFA energy in both diets. The sum of carbohydrate, protein, and fat accounted for approximately 90% of the faecal energy measured by bomb calorimetry; small amounts of faecal energy seemed to be of another origin.
Discussion
Results regarding the effect of MCT treatment on faecal output are conflicting19-21 but MCT is generally considered to reduce faecal loss of water and electrolytes and improve nutritional status in short bowel patients (Winawer et al, 1966 (one patient)22; Zurier et al, 1966 (two patients)23; Bochenek et al, 1970 (seven patients)24; Tandon et al, 1972 (three patients)25). This study indicated that a preserved colon in continuity was decisive for the efficacy of MCT therapy on absorption of energy and that MCT tended to increase output volumes in patients with a jejunostomy or ileostomy.
A colon in continuity was associated with a significant improvement in the absorption of MCFAs (fig 2). The excretion of MCFAs during MCT therapy was without exception low in patients with a colon, resulting in a universally high absorption of MCT even in patients in whom the absorption of LCT was negligible (fig 3). In contrast, the absorption of MCT was eventually impaired in the patients with the very low levels of LCT absorption and no colon. The distinct differences between the absorption of MCFAs in patients with and without a colon vanished for fatty acids with longer chain lengths, and patients with and without a colon had equally low levels of absorption of LCFAs, probably occurring in the small bowel only.
In patients with a preserved colon the replacement of dietary LCT by MCT consequently caused a considerable improvement in fat absorption, which resulted in a gain in total energy absorption, verifiable by bomb calorimetry (table 2). By contrast, the clinical efficacy of MCT with respect to overall energy absorption in patients with jejunostomy or ileostomy was so small as to be not measurable. This was because the replacement of half of the dietary LCT by MCT improved absorption of fat (MCT+LCT) less in patients with no colon (from 37% to 46%, p=0.05; table 2) than in patients with a colon (from 23% to 58%, p<0.001; table 2), and because MCT decreased the absorption of other nutrients as protein (from 63% to 51%, a difference of 0.443 MJ/day, p<0.05) and carbohydrate (from 71% to 63%, a difference of 0.252 MJ/day, p<0.05; table 2) in patients with no colon. Measured in absolute energy, the LCT+MCT diet increased fat absorption by 0.899 MJ/day in patients without a colon and by 2.079 MJ/day in patients with a colon (table 2), which should be evaluated against the fact that the LCT+MCT diet contained approximately 0.900 MJ/day more energy than the LCT diet. MCT also decreased the percentage of absorbed dietary LCT from 35% to 27% (p<0.05) in patients with jejunostomy or ileostomy. This unsuitable effect on protein, carbohydrate, and LCFA excretion was not significant if the colon was present, and might be due to the tendency of MCT to increase jejunostomy or ileostomy outputs.
Two arguments may be put forward to explain the improved MCT absorption associated with the presence of a large bowel. The more simple and likely explanation is that MCFAs, like SCFAs, are absorbed in the large bowel, possibly because they share water solubility characteristics, in contrast to the insoluble lipophilic LCFAs. Colonic absorption of water soluble fatty acids would be in accordance with the complete absorption of C8:0 and almost equally complete absorption of C10:0 (both water soluble at physiological pH), and the rapid decline in colonic influence on the absorption of fatty acids with increasing chain length (fig 3). A more speculative explanation is that the colon has a backward effect on fat absorption in the small bowel. Such a mechanism would probably result in an increase in the absorption of both MCT and LCT, and does not explain how four patients with a preserved colon could present with a lack of absorption of LCT and at the same time completely absorb MCT (fig 3).
Replacement of LCT by MCT often has to be limited to within 50% of total fat and a substantial supply of MCT may result in a diet high in LCT. Doses of MCT are usually kept considerably lower than in this study, inevitably decreasing the quantity of energy gained from MCT absorption. However, if the clinical goal is to increase energy absorption by 10–20% in a short bowel patient eating 10 MJ/day, one has to replace 1.5–3 MJ/day of LCT with MCT in patients who absorb 25% of LCT and 95% of MCT and other nutrients as usual, as was the average for the patients with a colon. A substantial effect is obviously more difficult to obtain if the difference between LCT and MCT absorption is less, as in patients with low grade malabsorption of LCT or in patients without a colon, in whom the benefit from MCT furthermore seemed to be jeopardised by increased malabsorption of other nutrients. High carbohydrate diets are an alternative way of optimising energy uptake in short bowel patients with preserved colonic function, because colonic fermentation converts malabsorbed carbohydrates to absorbable SCFAs.1 However, the high volumes of carbohydrate meals and colonic gas may hinder patients in consuming enough food and hyperphagia, which is an important way to compensate for severe malabsorption.26 MCT is a more dense source of energy, is not associated with gas production, and may be useful in optimising enteral energy absorption in short bowel patients with a preserved colon.
In summary, the short term clinical consequence of replacement of LCT with MCT in patients with small bowel resection and a jejunostomy or ileostomy was a comparable low increase in fat absorption, which was counterbalanced to the level of no effect on the overall energy balance due to a negative effect on the absorption of carbohydrate and nitrogenous substances. By contrast, MCT was almost completely absorbed in patients with preserved colonic function and resulted in a definite increase in fat and overall energy absorption in this subset of patients. It is suggested that MCFAs share the ability of SCFAs to be absorbed by the large bowel, and that the colonic digestion of malabsorbed carbohydrates and protein recently recognised to occur in short bowel patients1 ,2 is extended to include malabsorbed medium chain fat.
Acknowledgments
The technical assistance of Jette Christiansen, Anne Birgitte Larsen, Birthe Stenbæk Hansen, Kirsten Ahring, and Anne-Marie Raabyemagle is greatly appreciated.