Article Text

Statistics from Altmetric.com
Climate change has been described as the biggest global health threat of the 21st century1 and has significant implications for gastrointestinal (GI) health and disease,2 which is the focus of this consensus commentary provided by the World Gastroenterology Organisation (WGO) Climate Change Working Group (CCWG). The CCWG has members from 18 countries representing high-income, medium-income and low-income populations. The WGO includes gastroenterology societies from 108 countries, which represent more than 60 000 medical practitioner members. The CCWG members, who have coauthored this consensus commentary, aim to review the scientific literature on climate and GI health, to encourage education and the undertaking of actionable measures including advocacy, and to further research and collaborations within the global GI community. The CCWG’s objective is to assist GI health providers worldwide to adapt to, and mitigate, the effects of climate change on health. The CCWG has partnered with three major GI journals, which are copublishing this commentary, given the timeliness and importance of the topic.3 4
Overview of the impact of climate change
Climate change
The earth’s climate is changing because of increasing concentrations of greenhouse gases in the atmosphere, which has already warmed by more than 1°C compared with preindustrial times. The aim of mitigation efforts is to keep the rise in global mean surface temperature (GMST) below 2°C by 2100. An increase of 2°C might not seem like a major change, but variations of similar magnitude have been associated with profound alterations of climate in the past. It is important to note that even if this somewhat arbitrary target can be met, catastrophic changes in earth ecosystems can still occur.
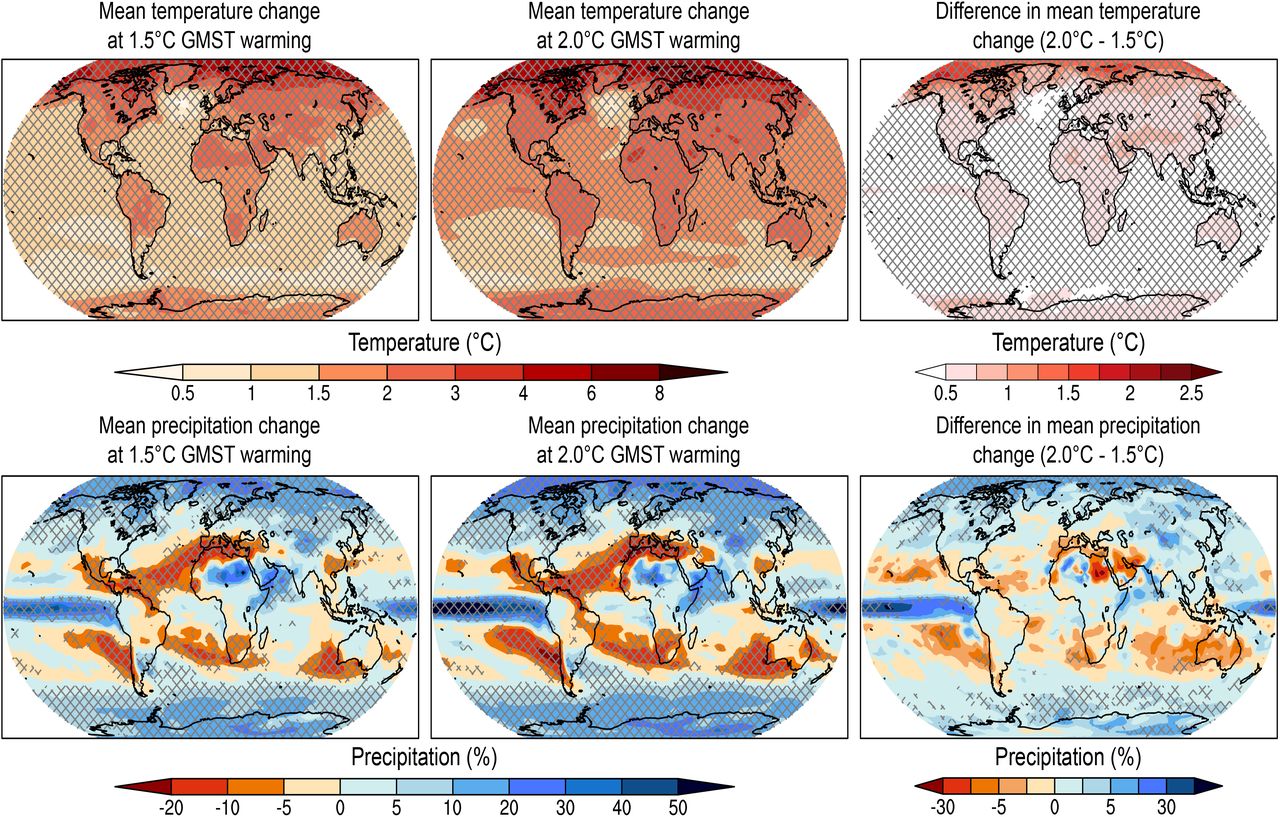
The Intergovernmental Panel on Climate Change was established in 1988 with a mandate to assess relevant scientific literature related to climate change. It produces regular reports and updates about climate change. The Intergovernmental Panel on Climate Change projects that as GMST rises, warming will be more pronounced in some areas than others (figure 1). For example, as global average temperature reaches +2°C, temperature in the Arctic may exceed +5°C. The changes in atmospheric temperature, moisture content and movement will lead to shifts in rainfall, with decreased or increased precipitation depending on the region (figure 1). This has implications for access to 2 of the fundamentals for life and health: water and food. Mean temperature change is one metric of temperature change. From a health perspective, other measures, such as the number of days with a maximum temperature greater than the 90th centile are likely more important than the yearly GMST average. Similarly, average changes in precipitation might not be meaningful if rainfall arrives at the wrong time for planting crops. In addition to climate change, other components of the planetary health framework, namely biodiversity loss and toxin exposure, need to be incorporated into considerations of the future of GI and liver health.5 Other key parameters of GI and non-GI health include food, water, infrastructure security, biodiversity, changing patterns of GI infections and migration.2

Maps of mean temperature and precipitation change at +1.5°C and +2.0°C GMST (global mean surface warming) and the difference between the 2. Greater temperature changes are seen over land masses and in northern latitudes. Bands of decreased precipitation are seen in both southern and northern hemispheres with increased precipitation closer to the poles. The cross hatching highlights areas where at least two-thirds of climate models agree on the sign of change as a measure of robustness. From Hoegh-Guldberg et al,13 reprinted with permission from the Intergovernmental panel on climate change.
Biodiversity
Biodiversity is the variety of life, including variations in genes, species and functional traits. It is more difficult to link changes in biodiversity, as opposed to direct effects like droughts, to human health because the effects are indirect. The diversity of life on land and ocean is in rapid decline. This is problematic, as greater biodiversity contributes to increasing crop yields, stabilising fisheries, fodder yield, pest control, plant disease resistance, climate modulation, water purification and pollination.6 Biodiversity loss is associated with increased risk of pathogen transmission,7 including viral epidemics.
Pollution, toxins and chemical exposure
The increase in food production during the last several decades was driven in part by agrochemicals. In fact, two-thirds of global agricultural land is now at risk of pesticide pollution.8 These chemicals are found on food for sale, are biologically active in humans, metabolised in part by gut microbiota, and capable of altering gut flora.9 There is also a wide variety of biological toxins that are climate sensitive. Mycotoxins are naturally occurring toxins produced by fungi, which have been linked to a variety of illnesses, including hepatocellular carcinoma.10 Warm, moist, storage environments and consumption of foods of marginal quality increase the risk of exposure. Algal blooms are associated with nitrogen and phosphate contamination of fresh water. Cyanobacteria can produce toxins that are nephrotoxic and hepatotoxic.
Nutrition
In both low-income and high-income countries, malnutrition from undernutrition and obesity are simultaneously problematic. More than half a billion people are undernourished. This number will grow as crop yields decline in a warming world, while populations continue to increase.11 Furthermore, rising temperatures and atmospheric CO2 may decrease the nutritional value of some crops. Decreasing crop yields of lower nutritional value will exacerbate the existing problems of undernutrition, wasting, stunting and micronutrient deficiency, and paradoxically might drive an increase in obesity, as mild to moderate insecurity has been linked to higher obesity rates,12 which is likely to contribute to an increase in nonalcoholic fatty liver disease and metabolic-associated fatty liver disease.
Food production contributes as much as 25% of global greenhouse gas emissions. In addition, concerns have been raised regarding the loss of biodiversity from conversion of wilderness to farmland, and the use of pesticides and fertilisers. Attention has also focused on beef and dairy industries because cattle are a source of the potent greenhouse gas methane.
Water
Nearly 40% of the world’s 7.9 billion people live in areas with high to very high water shortages or scarcity. Just as crop yields fall as temperatures rise, so also does access to clean fresh water. Pesticide, chemical use and contamination with sea water threaten the quality of water available. Utilisation of water of questionable quality increases the risk of exposure to toxins and infections.
Rising CO2 in the atmosphere, the primary driver of climate change, dissolves in the oceans and increases acidity, interfering with the ability of shellfish, coral and some plankton to form their shells and skeletons. Ocean temperature, chemical change and overfishing will lead to a decline in this important source of nutrition.
Changing patterns of GI disease
The incidence of many GI diseases, such as inflammatory bowel disease and colorectal cancer, show marked geographic variation, in part due to environmental factors. It can be anticipated that epidemiological shifts in GI disease will occur with a changing environment. There is also a close link between mental health and functional GI disease. Populations are already subject to chronic stress because of struggles to obtain food, water and shelter. Acute stress from events such as wildfires, floods and storms, and from forced or elective migration, will add to this mental health burden. An increase in functional GI disorders can be anticipated as climate threats increase.
Two-thirds of the world’s megacities are located by the sea. The number of people impacted by sea level rise will depend on the degree of temperature rise. Without adaptation measures, more than 100 million people will be affected by 2050.13 Displacement of many of their inhabitants, and the risks from storm surges, will add to the populations forced to migrate because of global warming. Climate change will increase migration as populations move from areas experiencing water and food stress, both from rural to urban areas and between countries. The health needs of these groups and their ability to access care, vary widely depending on their migrant status and the stage of the migrant journey.14 15 GI healthcare providers will need training in diagnosis and management of diseases with which they might not be familiar and in the cultural differences with which different groups approach healthcare needs.
Diarrhoeal illnesses consistently rank in the top five categories of global disease burden,16 even before the exacerbating effects of climate change. Transmission of infectious agents to humans depends on pathogen, vector and host interactions and occurs in a social context. Climate change alters these relationships through changes in temperature, humidity, habitat, access to clean water, food and sanitation, and is predicted to bring major changes in the epidemiology of infections.17 Both high and low rainfall extremes are associated with an increased risk of GI infections, even in higher-income countries.18 High rainfall events can lead to contamination of reservoirs with water containing surface organisms and can also overwhelm wastewater treatment. Low rainfall leads to use of water of marginal quality, concentration of pathogens, and reduced sanitation flow. Global warming is also affecting the geographical range of a wide variety of GI infections. One example is the change in the range of Vibrio cholerae. Formerly seen in high-income countries rarely, changes in the temperature of the oceans have led to the appearance of cholera along the northwestern seaboard of North America and in the Baltic.19
The main impact of climate change on the liver will likely be changes in the prevalence of metabolic liver disease secondary to changes in nutrition, increased risk of hepatitis A and E from flooding, changes in the geographical distribution of other liver infections, such as schistosomiasis, and exposure to toxins, such as aflatoxin.
Acute heat exhaustion has well-described multiorgan effects, including digestive organs. Less is known about the effect of chronically elevated temperatures on intestinal function. A warming atmosphere holds more energy and water. Storms are expected to increase in severity and possibly increase in frequency. GI care is heavily dependent on functioning infrastructure. Storms, wildfires and floods are already impacting care, and this will likely increase. Planning for adaptive measures to limit the impact of these events should proceed with urgency.
Although the focus of this commentary is on GI health, the health challenges of the changing environment will affect every organ system. Understanding the effects of climate change, biodiversity loss and toxin exposure on organ systems other than the gut and how that can relate to intestinal function is in evolution.
Carbon footprint and non-recyclable waste
The health sector and all of us as individuals are significant contributors to greenhouse gas emissions, the majority of which is CO2, but also includes methane, nitrous oxide and hydrofluorocarbons. Formation and retention of greenhouse gases in the atmosphere lead to increased energy that translates to global warming due to higher air and water temperatures. The ‘carbon footprint’ represents the CO2 equivalents that are produced, be it by the burning of fossil and biofuels or use of electricity, heating and cooling, transportation, food and consumer goods. In the USA, health services account for as much as 8% of total national carbon emissions. The nature of our GI specialty leads to a significant contribution not only to the carbon footprint, but also to huge amounts of non-recyclable plastics waste.20 21
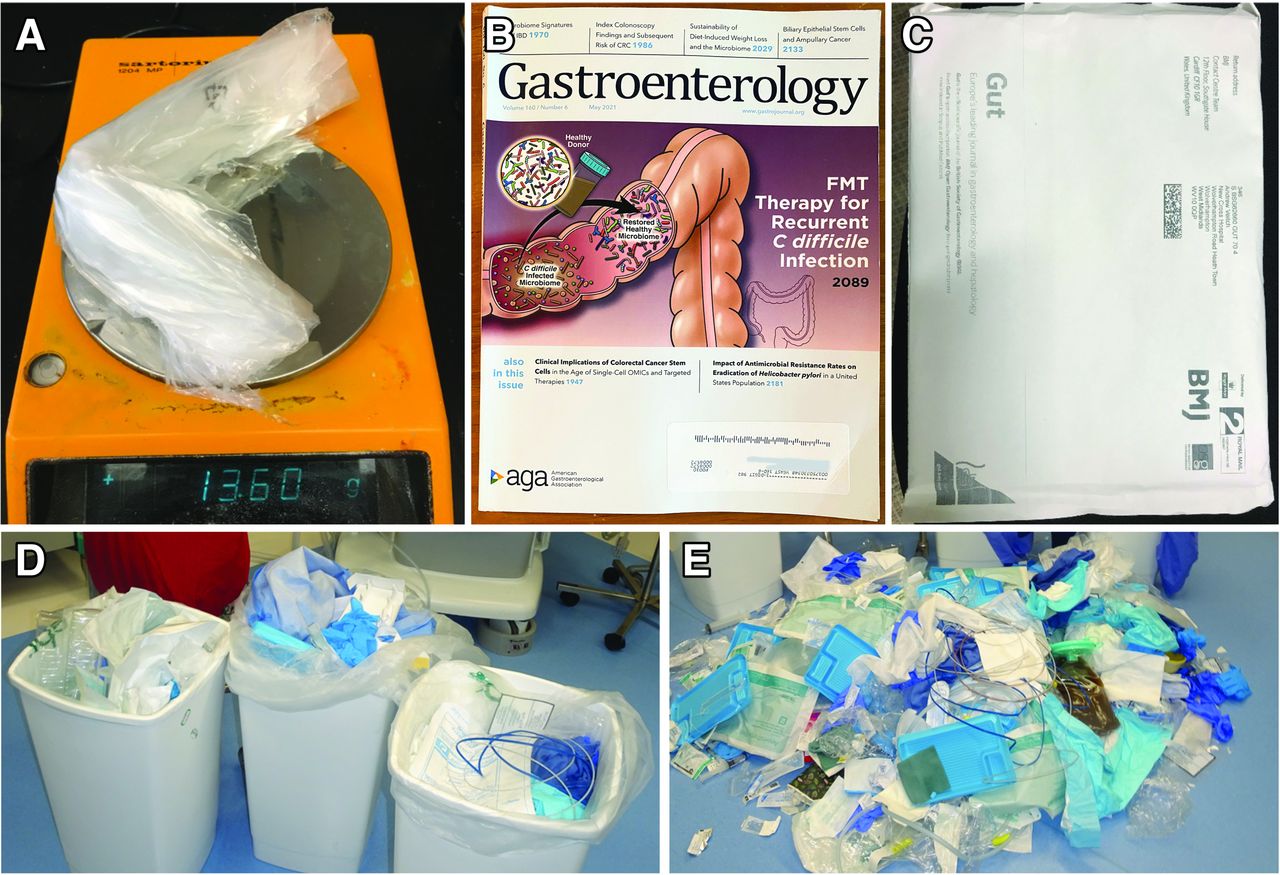
Plastic waste also comes from many of the nearly 15 000 medical journals, although the fraction of online journals is increasing. Many digestive health and disease journals continue to have plastic covers. The impact of plastic journal covers of two journals published by the American Gastroenterological Association alone represented 1.4 metric tons annually (figure 2A, extrapolated to the journals published by American Gastroenterological Association that are mailed to its members). Of note, journals affiliated with the American Gastroenterological Association and British Society of Gastroenterology have converted the use of plastic covers to labels or to paper covers (figure 2B,C).
{kind=link}
{kind=link}
Conversion of plastic Journal covers to paper, and waste generated by endoscopy procedures. (A) The plastic covers of two typical journals weigh 13.6 g; (B, C) some of the major GI journals have switched from using plastic covers to either paper labels (Gastroenterology) or a paper cover (Gut). (D) Three bins of endoscopy-generated waste from an endoscopy unit in Melbourne, Australia (for nine colonoscopies with polypectomies and one upper endoscopy, excluding the suction and drainage tubing and canisters). The bins shown in (D) were then weighed after emptying their contents (E). The net weight of waste per procedure was 0.54 kg. GI, gastrointestinal.
The plastic waste from endoscopic procedures is also difficult to fathom. For example, one endoscopic procedure can be estimated to generate 0.54 kg of waste (eg, figure 2D,E), although the non-recyclable plastic waste levels become 1.2 kg if suction canisters, tubing and other accessories are included.21 Therefore, for 11 million estimated colonoscopies carried out in the USA,22 the approximate non-recyclable plastic and non-plastic waste in the USA from colonoscopies alone is nearly 13 200 tons. Similarly, digestive organ endoscopy was reported to be the second highest procedure-associated waste-generating medical department (0.50 kg/procedure) after radiology (0.67 kg/procedure), with plastic surgery being third (0.44 kg/procedure).23 Notably, plastics can also be degraded to form microplastics, composed of plastic particles <5 mm in size, which can be detected in marine shores and even in human colectomy specimens.24 Specific measures to curtail the pollution impact that is generated by the care provided by gastroenterologists will be discussed.
What measures should be undertaken by the gastroenterology community?
The WGO leadership made the strategic decision to establish a CCWG because of the global impact of climate change as discussed and the need for grassroots efforts. Several medical organisations have begun to form climate change focus groups or consortia, such as The Medical Society Consortium, which includes 19 society members.25 We believe that individual GI member societies can act locally and think globally and can be highly effective, given that the needs and resources vary widely across and even within countries. As such, GI societies can be involved directly and indirectly with almost all of the specific efforts, and so can endoscopy centres, GI practices, academic centres, publishers and individuals (table 1). In general terms, the efforts revolve around reducing the level of greenhouse gas emissions, curbing non-recyclable waste and working toward developing affordable, climate-friendly, substitute disposables.
What can global gastroenterology societies, endoscopy centres, practices, publishers, individuals and academic centres do to support planetary health?
Measures that can be taken to address the challenges can be adaptive or designed to mitigate. Adaptive measures do not aim to alter the course of climate change but to build resilience. Mitigation efforts are designed to reduce greenhouse gas emissions with an ultimate aim of a carbon neutral environment by 2050.
The initial goals of the WGO CCWG, which we encourage other gastroenterology member societies to establish and undertake, include the following:
Advocacy, by publicly supporting efforts of member GI organisations within their countries, be it to support environment-friendly laws or to support increased funding, or to support efforts similar to those that the National Health Service has undertaken.26
Education and information, by establishing a website that will house education material and relevant publications; hosting of webinars and podcasts; including climate change sessions at WGO meetings; assembling content and topic interested subgroups of the CCWG and involving other WGO members to develop consensus statements and other in-depth analyses that examine the health impact of climate change in a continent or region of the world; assess topics such as reusable endoscopy equipment, reducing greenhouse gas emissions from hospitals or institutions, redesigning educational activities to minimise the carbon footprint, including relevant content in the curricula of medical schools; and approach publishers in relation to reducing greenhouse gas emissions in the publication industry.
Collaboration with gastroenterology member societies and other medical organisations. One major aspect of this is to work together to decrease the carbon cost of the annual and other sponsored conferences, much of which is related to air travel that could be mitigated by hybrid in-person and remote meetings and other measures.27 28 In this regard, the COVID-19 pandemic has already taught us that we can very effectively carry out major international virtual meetings. Industry also has an important role to play in helping reduce the carbon footprint of gastroenterologists by reducing waste, exploring the possibilities for reusable equipment and helping to promote virtual and hybrid conferences.
These steps will contribute to mitigation of the climate crisis through reduction of greenhouse gases and will inform strategies for adaptation to the changes that are underway. For its share, the WGO CCWG will be conducting a survey of its members and developing a strategic plan for WGO to follow within the organisation and externally along the lines highlighted above. In addition, the African Middle East Gastroenterology Association is establishing a Climate Action Group, the Canadian Association of Gastroenterology has a special interest section, and the British Society of Gastroenterology Working Group on Climate Change and Sustainability is undertaking similar strategic planning efforts. It is an opportune moment for the medical community to work together to proactively tackle planetary health challenges as they grow exponentially.
Knowledge gaps
Research is critically needed in several areas.29 Priorities include the clinical impact of the changing climate and rising temperatures on GI health, the relationship between acute and chronic climate stress on functional disorders, the impact on gut microbiota of environmental toxins and decreasing biodiversity, and the role of microplastic exposure on gut health and nutrition. Strategies for endoscopy centres are central to gastroenterology practice,29 30 as are development of affordable disposable plastic substitutes, how best to educate GI healthcare providers, and how to translate knowledge about the climate threat into effective action.
As noted above, climate change has different impacts on health in different regions of the world. The WGO CCWG is setting up subcommittees comprising gastroenterologists from different regions around the world to research and report about the impact of climate change on health in their regions.
Summary
Human progress during the last 100 years came at a huge cost to the environment. As we face the challenge of a warming climate, many measures of GI health are already problematic. The impact of climate change will be felt most severely in lower-income countries, which already struggle to deliver care. Climate change will pose significant additional burdens on digestive health and disease. Meeting this challenge within our specialty, while providing the best preventive; diagnostic and therapeutic GI population care, will necessitate a unified global approach to rectify the current impact of climate change and non-recyclable waste.31 We close with quotes from three leading world figures, a politician, a cleric, and an 18-year-old activist. ‘By polluting the oceans, not mitigating CO2 emissions and destroying our biodiversity, we are killing our planet. Let us face it, there is no planet B’ (Emmanuel Macron); ‘We only have one world. If we destroy it, we’re done for’ (Desmond Tutu); and ‘The eyes of all future generations are upon you. And if you choose to fail us, I say—we will never forgive you’ (Greta Thunberg).
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Sarah Williamson and Sunni Losito (American Gastroenterological Association) for assistance with figure preparation, and members of the World Gastroenterology Organisation (WGO) executive committee for reviewing and approving the content of this commentary. The authors also thank Marissa Lopez and Jim Melberg for their support of the WGO Climate Change Working Group, Professor Anthony Capon, Director, Monash University, Sustainable Development Institute, for reviewing our manuscript, and Associate Professor Andrew Metz, Director of Endoscopy, Royal Melbourne Hospital, for kindly providing the images and related information displayed in figure 2D and E.
References
Footnotes
Presented at This article is being published jointly in Gastroenterology, Gut and Journal of Clinical Gastroenterology. The article is identical except for minor stylistic and spelling differences in keeping with each journal’s style. Citations from any of the 3 journals can be used when citing this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Author note All authors contributed to the concept, content and final text, and review of the work, with the first five authors playing a lead role.