Article Text

Abstract
Background Anti-tumour necrosis factor (anti-TNF) therapies are the most commonly used biologics for inflammatory bowel disease (IBD), but for patients with a comorbidity, newer agents may be a more appropriate treatment choice.
Aims To investigate the impact of comorbidities in patients with IBD, on first-line biologic prescribing habits of IBD-specialist healthcare practitioners in the UK.
Methods IBD-specialist physicians and nurses were asked to answer an online survey, considering different prescribing scenarios in ulcerative colitis (UC) and Crohn’s disease (CD). Respondents could indicate a preference for anti-TNFs or newer biologics, both in the absence and presence of 10 common comorbidities.
Results A total of 120 IBD-specialist healthcare professionals (HCPs) completed the survey. In the absence of comorbidities, anti-TNFs were favoured; infliximab was the preferred first-line biologic in both UC and CD (43% and 37% of respondents, respectively). On introducing comorbidities, the largest shift in prescribing behaviour was for vedolizumab, with preference increasing by 27% and 21%, compared with infliximab, which fell by 14% and 9% in UC and CD, respectively. Chronic/recurring infection (46%), congestive heart failure (≤44%) and malignancies (≤43%) were the most commonly selected comorbidities for vedolizumab treatment.
Conclusions Clinicians adapt their biologic prescribing habits in patients with IBD with comorbidities, considering known contraindications and precautions. A preference for vedolizumab is evident in many cases, however, for several comorbid scenarios, including demyelinating disorders, chronic obstructive pulmonary disease and malignancy, anti-TNFs are prescribed despite known risks. It is important that continual re-evaluation of the IBD treatment landscape is undertaken by HCPs, in alignment with recommendations in published guidelines.
- crohn's disease
- inflammatory bowel disease
- colorectal cancer
- functional bowel disorder
- IBD clinical
Data availability statement
Data available within the article or its supplementary materials. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Although anti-tumour necrosis factor (anti-TNF) therapies provide good efficacy in ulcerative colitis and Crohn’s disease with an established safety profile, contraindications and precautions (eg, prior infections, severe heart failure, history of demyelinating disease/malignancy) can limit their use.
Newer biologic classes, such as anti-integrins (ie, vedolizumab), anti-IL-12/23s (ie, ustekinumab) and Janus kinase (JAK) inhibitors (ie, tofacitnib) offer alternative efficacy and safety profiles to anti-TNFs.
What this study adds
This survey study provides insights into the impact of common comorbidities on first-line biologic prescribing preferences in inflammatory bowel disease (IBD) in the UK.
Overall, clinicians adapt their biologic prescribing habits in patients with IBD with comorbidities, considering contraindications and precautions, although in some situations, anti-TNFs are prescribed despite the known risks.
How might it impact on clinical practice in the foreseeable future
This study highlights the need for continual re-evaluation of the IBD treatment landscape by healthcare professionals in alignment with recommendations in published guidelines.
Introduction
The treatment landscape for inflammatory bowel disease (IBD) in the UK is ever evolving as options become available with differing mechanisms of action.1 Used for over a decade, anti-tumour necrosis factor (anti-TNF) therapies are licensed for the treatment of patients with IBD refractory to conventional therapy. Three newer biologic classes, anti-integrins (ie, vedolizumab), anti-IL-12/23s (ie, ustekinumab) and Janus kinase (JAK) inhibitors (ie, tofacitnib), have entered the therapeutic landscape. These agents offer alternative efficacy and safety profiles to those of anti-TNFs.
While anti-TNFs are widely used, providing good efficacy in ulcerative colitis (UC) and Crohn’s disease (CD) with an established safety profile,2–4 reported contraindications and precautions can limit their use. Prior occurrence of infections, severe heart failure, history of demyelinating disease and a history of malignancy should all be taken into account before prescribing anti-TNFs.5–7 Additionally, there are issues with secondary loss of response due to immunogenicity with an incidence between 23% and 46% at 12 months after anti-TNF initiation.6 Consequently, combination therapy with an immunomodulator such as azathioprine is frequently prescribed in order to maintain remission.8 Both thiopurine monotherapy and anti-TNF monotherapy significantly increase the risk of lymphoma, and the risk is greater with combination therapy.
Ustekinumab provides an alternative biologic option to anti-TNFs, having demonstrated efficacy and safety in the UNITI and UNIFI registration trials.9 10 Vedolizumab is a further option, having demonstrated efficacy and safety in the GEMINI trials,11 and in a growing body of randomised controlled trials and real-world findings,12–17 offering a gut-selective mechanism of action in contrast to the systemic activity of both anti-TNFs and ustekinumab.
Comorbidities tend to be under-represented in clinical trials and patients with severe comorbidities are usually excluded.18–20 Prescribing advice is typically based on expert opinion or real-world observational studies. The limited literature addressing comorbidities in IBD focuses on anti-TNFs. Given this lack of evidence and guidance, it is helpful to understand how clinicians take comorbidities into account. In this study, we employed a survey to understand the impact of common comorbidities on first-line biologic prescribing preferences in IBD in the UK.
Methods
Identifying comorbidities
A list of 22 comorbidities relevant to biologics in IBD was compiled, based on published literature, contraindications, author insights and clinical experience. The 10 most clinically relevant comorbidities overall were then selected for inclusion. These were malignancies, elderly patients, hepatitis B/C, chronic/recurring infection, chronic obstructive pulmonary disease, congestive heart failure, demyelinating disease, transplant, liver disease, arthropathy (seropositive). The elderly population typically encompasses a range of different comorbidities but has been considered for this study as a collective term.
Survey development
An online survey was developed to elicit UK biologic prescribing patterns for IBD, in which respondents considered a range of prescribing scenarios in the absence and presence of comorbidities. Biologic options for selection were randomised in each question to investigate use of adalimumab, infliximab, vedolizumab, golimumab and ustekinumab in IBD (tofacitinib not considered as not approved at time of survey). Respondents could choose biologics either as monotherapy or in combination with an unspecified immunomodulator and asked to consider adult patients with moderate to severe UC/CD, basing their decisions on a clinical perspective (ignoring influence due to cost, or due to local prescribing rules restricting certain options).
Survey design
The survey addressed preferences for first-line biologic prescribing in the absence of comorbidities and subsequently with comorbidities. The sequence of comorbidities shown and, within each comorbidity, the order in which UC or CD was displayed were randomised.
Survey recruitment
Of 2000 members of a market research panel matching the inclusion criteria, the first 100 physicians and 20 nurses to respond to the survey were included in the study. Healthcare professional (HCP) qualifications were verified by a rigorous screening process prior to survey start, followed by additional screening questions to ensure a minimum of 3 years as an IBD specialist with seeing at least 10 patients/month with IBD.
Results
Survey respondents
The survey was completed in November 2018 with 120 healthcare practitioners. The majority of nurses saw at least 21 patients per month (55%–60%); physicians mainly fell into the ‘11–20’ and ‘21 or more’ patients per month categories (table 1).
Demographic characteristics of IBD specialists responding to survey (n=120)
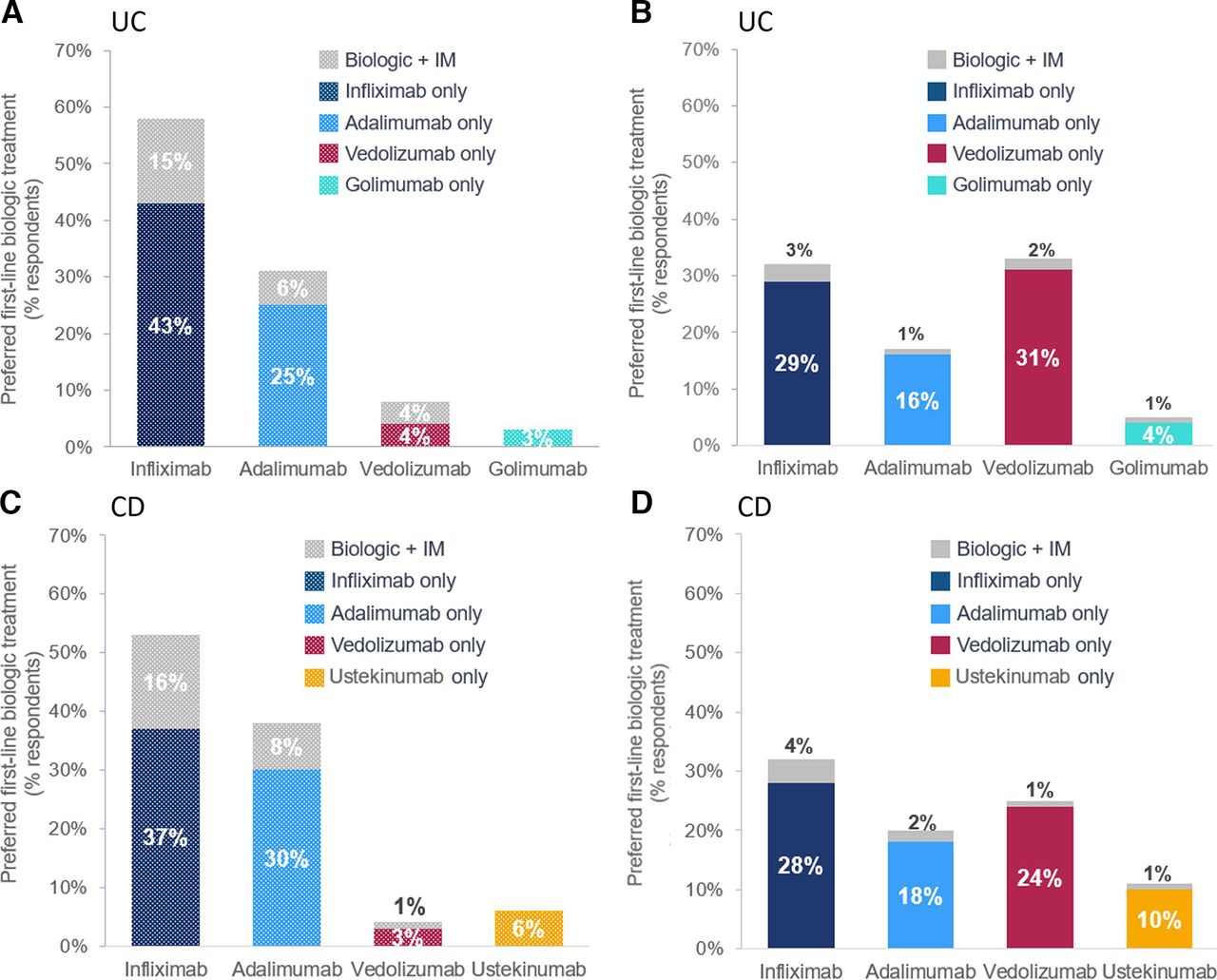
Patterns of biologic prescribing in the absence of significant comorbidity
In the absence of comorbidities, there was a wide variation in use of biologics (figure 1). Anti-TNFs were reported to be most commonly prescribed in biologic-naïve patients with UC and CD without comorbidities; infliximab specifically was the most commonly prescribed anti-TNF for UC and CD, for 43% and 37%, respectively, closely followed by adalimumab for both UC and CD (25% and 30%, respectively).

Preferred first-line biologic treatment in the scenario of moderate to severe UC and CD adult patients with no comorbidities (A and C respectively), compared with the presence of comorbidities (B and D respectively; mean preferences measured across all comorbidities). Total sample, n=120; IBD-specialist physicians n=100, IBD-specialist nurses n=20. Question: Please consider the following patient case where conventional therapies (eg, immunosuppressants, steroids) have not worked or are not suitable. What would be your preferred first-line biologic treatment choice when no comorbidities are present, either as a monotherapy or in combination with an immunomodulator, in this case? Respondents were always asked to answer the questions from a purely clinical perspective. CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis.
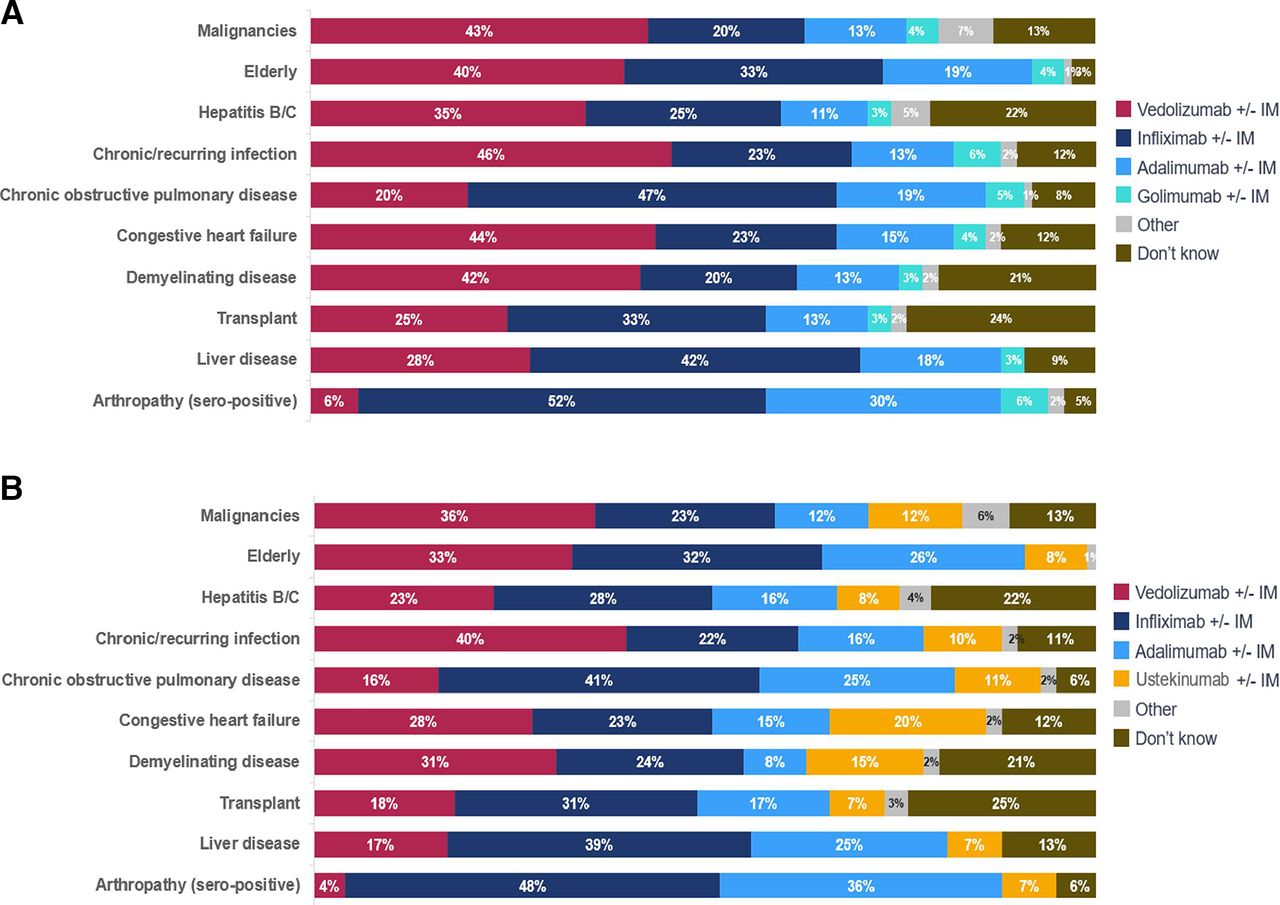
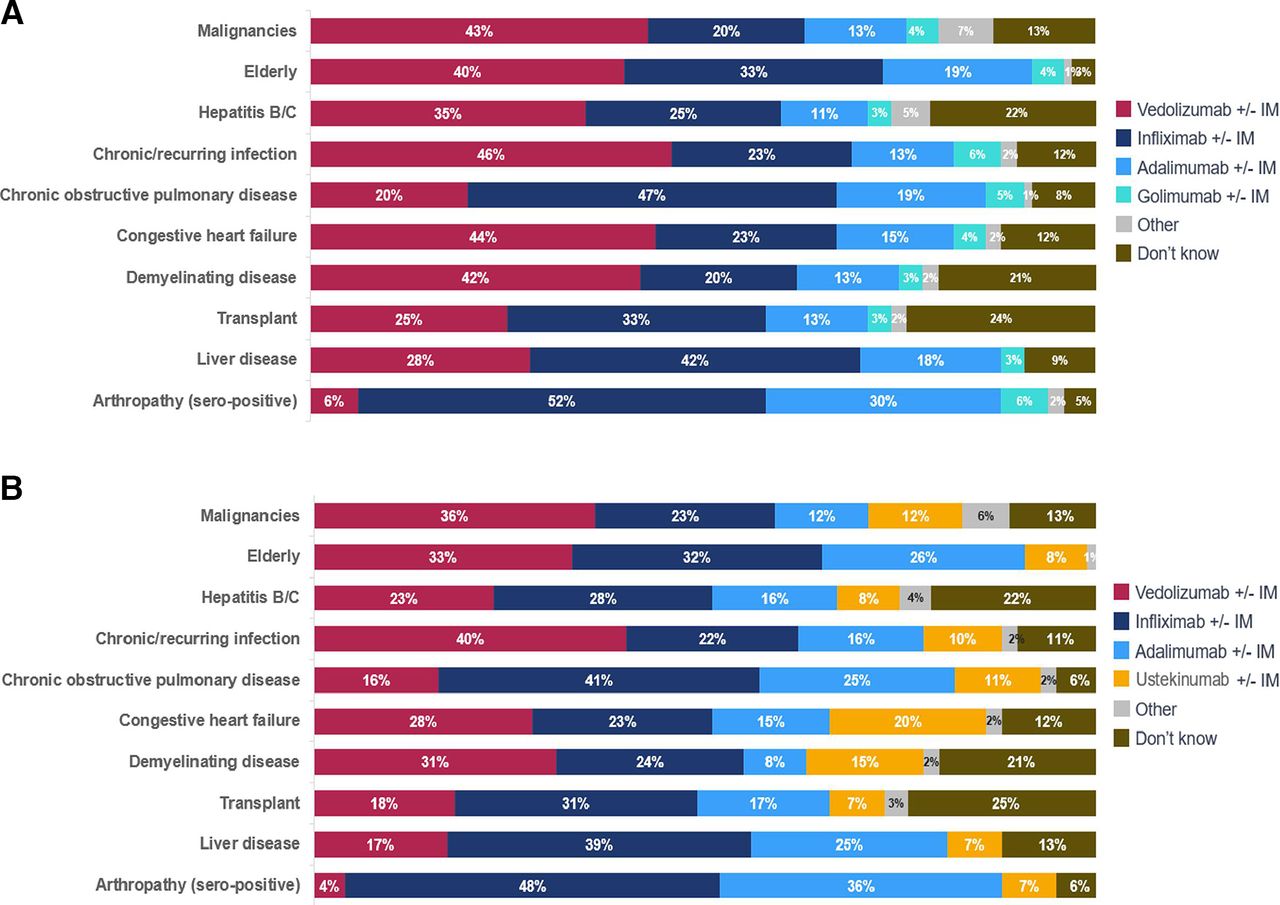
Preferred choice of biologic in the presence of comorbidities
When the 10 comorbidities were introduced into the survey, there was a shift in pattern of practitioners’ prescribing habits for first-line biologics, affecting both UC and CD. A change in preference for vedolizumab was evident, increasing choice by 21%–27% for use across CD and UC in the presence of comorbidities, whereas the preference for infliximab reduced by 9%–14% across CD and UC (figure 1).
In UC, vedolizumab was the foremost preferred first-line biologic treatment choice for 6 of the 10 comorbidities investigated (figure 2). Infliximab was favoured for the remaining four comorbidities in UC; most pronounced for arthropathy (up to 52%) (figure 2). In CD, the prescribers' preference for infliximab compared with vedolizumab as a first-line biologic with each as first preference for five comorbidities (figure 2).
{kind=link}
{kind=link}
Preferred first-line biologic treatment in the scenario of moderate to severe UC (A) and CD (B) in adult patients with comorbidities. Preferred first-line biologic treatment choice in the presence of individual comorbidities for moderate to severe UC (A) and CD (B), adult patients (note comorbidities are presented in order of author ranking with the foremost selection listed first). Total sample, n=120; IBD-specialist physicians n=100, IBD-specialist nurses n=20. Question: What is your first-line biologic treatment choice, either as a monotherapy or in combination with an immunomodulator, assuming this patient has UC/CD? What would be your preferred first-line biologic treatment choice when (xxxx) comorbidity is present, either as a monotherapy or in combination with an immunomodulator, in this case? Respondents were always asked to answer the questions from a purely clinical perspective. CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis.
In UC and CD, vedolizumab was the first-line biologic treatment choice for the comorbidities including chronic/recurring infection, elderly, malignancy and demyelinating disease (figure 2).
Uncertainties (‘don’t knows’) were common for transplant (24%–25%), hepatitis B/C (22%) and demyelinating disease (21%) across UC and CD. There was no correlation in first-line biologic treatment preference between the different years of experience classifications either for no comorbidity or comorbidity scenarios.
The use of an immunomodulator in combination with a biologic was preferred by a maximum of 4% in the presence of a comorbidity, whereas in the absence of a comorbidity, 16% preferred this approach.
Discussion
In the absence of comorbidities, treatment with infliximab was the preferred first-line biologic, in line with real-world data demonstrating the dominance of anti-TNFs in current prescribing, with an increase in vedolizumab use between 2015 and 2017.1 Adalimumab was the second-choice biologic, whereas the recent European Crohn's and Colitis Organisation (ECCO) guidelines recommend ‘vedolizumab rather than adalimumab for the induction and maintenance of remission in patients with moderately-to-severely active ulcerative colitis’ and, therefore, prescribing may change in favour of vedolizumab in future.21 When surveyed about prescribing choices in patients presenting with a comorbidity, we observed that clinicians adapt their prescribing.
While we observed appropriate decision-making for first-line biologic preference in patients with comorbidities taking contraindications and precautions/warnings for anti-TNFs into account, we were surprised to see decisions contrary to current advice. For example, prescribing anti-TNFs in patients with pre-existing demyelinating disorders has been associated with exacerbation of clinical symptoms2 and is strongly discouraged, yet over 30% of respondents chose anti-TNFs. Despite clinical evidence suggesting patients with chronic obstructive pulmonary disease (COPD) may be at increased risk of developing malignancy or recurrent infection22 if treated with infliximab, there was a marked preference for anti-TNFs as first-line biologic. This may be due to lack of dissemination but could be due to some controversy surrounding the data, so COPD is not seen as absolute contraindication to anti-TNF use. However, consideration should be given to the risk of malignancy in patients with COPD when prescribing biologics.
Anti-TNFs have also been associated with excess mortality in patients with heart failure yet are still widely prescribed based on these results.23 It is recommended that patients with a reduced ejection fraction, especially New York Heart Association (NYHA) class III and IV, should avoid anti-TNFs.24 Since our survey did not specify the NYHA class of heart failure, respondents may have based their answers on milder forms of heart failure, which are not an absolute contraindication. However, overall, a number of prescribers seem not to be considering current advice on anti-TNF prescriptions in these groups, possibly due to lack of awareness of these contradictions or because they are not convinced by the evidence.
It is notable that ustekinumab preference overall is relatively low likely reflecting its relative recent licensing at the time of the survey, limited availability of data and practitioner’s comfort with pre-existing prescribing habits for patients with CD. However, data from the Psoriasis Longitudinal Assessment and Registry has identified no increased risk of malignancy, major adverse cardiovascular events, serious infection or mortality with ustekinumab, suggesting that this option may also have a favourable safety profile in patients with IBD,25 although the dose of ustekinumab used for psoriasis is typically lower than for IBD. Furthermore, since the survey was conducted, findings from the SEAVUE study have added to the overall body of knowledge for ustekinumab in IBD.26
Vedolizumab is the first-line biologic of choice in the presence of malignancies, likely reflecting the contraindication and caution for use of anti-TNFs in patients with a history of cancer.1 24 27 Furthermore, anti-TNF therapy has been shown to increase the risk of lymphoma in patients with IBD and no history of cancer.8 However, for certain types of malignancy, there is some uncertainty in the literature regarding the link between anti-TNFs (both with and without immunomodulators) and malignancy, suggesting patients may be at no increased risk.28 29 This is mirrored by the ECCO (2015) consensus, stating that there is no obvious excess risk of developing a second (new or recurrent) cancer while treated with anti-TNF therapy.30 Interestingly, as patients with a history of cancer have usually been excluded from infliximab trials, there is limited evidence available associating anti-TNFs and history of malignancy.24 Nevertheless, it is biologically plausible that while blocking TNF does not cause malignancy, it may be permissive to malignancy that is already present. While the gut-directed mode of action of vedolizumab would indicate a favourable safety profile in the presence of malignancy, further clinical data are needed.
Anti-TNFs have been shown to be less efficacious in the short term and accompanied by a higher rate of severe adverse events in patients ≥65 years compared with younger counterparts, although some studies have not identified a difference between anti-TNFs and other classes of biologics.31 32 A greater risk of infection has also described in patients ≥65 years on anti-TNFs alone, or in combination with immunomodulators, although this may be attributable to the immunomodulators.33–35 A history of malignancy should be ruled out in elderly patients prior to initiating biologics since risk increases with age.24 36 A recent study revealed that gastroenterologists consider ustekinumab and vedolizumab more appropriate treatments than anti-TNFs in patients ≥65 years with a history of malignancy or serious infection.37 Despite these considerations for the elderly, over 30% of respondents showed a preference for infliximab.
In this study, vedolizumab was the preferred first-line biologic for patients presenting with chronic/recurring infection. Anti-TNF therapy in patients with IBD with latent infections can lead to flare-up of tuberculosis, viral infections such as HIV and varicella zoster virus.22 38–40 Vedolizumab therapy may, therefore, be more appropriate in these circumstances and all patients with IBD should be screened for latent infections prior to initiating anti-TNFs.37 Combination of biologics with immunomodulators is expectantly low due to their association with an increase in opportunistic infections, especially in combination with anti-TNFs.41 These findings are supported by recent clinical trials and postmarketing data showing that the rate of tuberculosis and serious opportunistic infections in patients receiving vedolizumab was low.35
Limitations to our study are first, the size of the cohort, although representative of UK IBD specialist doctors and nurses. Second, we cannot be sure that respondents were managing to dissociate their preferences from other non-clinical factors such as cost. Third, respondents may be influenced by restrictions on prescribing choices, based on guidelines. Fourth, we did not specify the severity of comorbidities, which may influence results.
In conclusion, this study suggests that HCPs adapt their prescribing of biologics to the presence of comorbidities. Since the survey was conducted, treatment options have expanded with ustekinumab licensed for use in UC in addition to CD. Tofacitinib, a small molecule of JAK inhibitor, is also approved for UC. There is a continued need to re-evaluate the treatment landscape for IBD in light of new studies, indications and currently unknown factors likely to affect prescribing habits as well as to provide education and training to HCPs and take on board other approaches, including personalised medicine.
Data availability statement
Data available within the article or its supplementary materials. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Medical writing support was provided by BioScience and survey development was conducted by Edelman Intelligence and distributed through M3 Global Research, all supported by Takeda.
References
Footnotes
Contributors AA, TO, NP, CS and CT developed the manuscript, with AA acting as the guarantor. All authors approved the final version of the manuscript. Edelman Intelligence collected data and medical writing support was provided by Edelman Editorial.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AK has received speaker fees and/or support to attend educational meetings from Janssen, Takeda, Dr Falk, Warner Chilcott, MSD, Abbvie and Vifor Pharma. TO has been a speaker at educational meetings sponsored by AbbVie, Allergan, MSD, Shield Pharmaceuticals, Takeda and Vifor Pharma; has participated in advisory boards sponsored by AbbVie, Allergan, MSD, Shield Pharma, Vifor Pharma and Biogen. NP has been an advisory consultant and/or speaker for Abbvie, Allergan, Astra Zeneca, Bristol-Myers Squibb, Celgene, DebioPharm, Dr Falk Pharma UK Ltd, Ferring, Galapagos, Janssen, Lilly, Pfizer, Takeda, Tillots, Vifor, and has received research grants from Takeda, Pfizer and Bristol-Myers Squibb. CS has received unrestricted research grants from Warner Chilcott, Abbvie, and Janssen, has provided consultancy to Arena, Galapagos, Warner Chilcott, Dr Falk, Abbvie, Takeda, Eily Lilly, Fresenius Kabi, Roche and Janssen, and had speaker arrangements with Warner Chilcott, Dr Falk, Abbvie, MSD, Pfizer and Takeda. CT has participated in advisory boards sponsored by Amgen and Takeda; has received support to attend educational meetings from Tillotts Pharma, and has received a charitable grant from Takeda.
Provenance and peer review Not commissioned; externally peer reviewed.