Article Text

Abstract
This review outlines the current classification of pancreatic cystic lesions, with a particular emphasis on pancreatic cystic neoplasms (PCNs). It will describe the diagnostic approach to PCNs, with reference to clinicopathological features, cross-sectional radiology and endoscopic ultrasound. This review will conclude with an evidence-based discussion of the management of PCNs focused on recent clinical guidelines.
- pancreatic disease
- pancreatic tumours
Statistics from Altmetric.com
Pancreatic cystic lesions (PCLs) are frequent incidental findings with modern cross-sectional imaging. The prevalence of cysts≥2 mm in imaging series is 4%–45%, increasing with age.1–3 The WHO 2010 classification of pancreatic tumours assigns PCL into four categories based on the presence or absence of an epithelialised cyst lining and neoplastic potential.4 Epithelialised neoplastic cysts include the pancreatic cystic neoplasms (PCNs), cystic degeneration of solid tumours and rarer tumours.4
Classification of pancreatic cystic neoplasms
Even in high volume centres, pancreatic surgery carries significant morbidity and mortality, and classification is key to establishing appropriate management or surveillance. Pseudocysts are an important benign differential, while malignant mimics include cystic neuroendocrine tumours and cystic degeneration of solid tumours.
In our experience (tertiary pancreaticobiliary cancer centre), we advise that most incidentally discovered or indeterminate aetiology PCLs are referred for central review and management discussion. The majority of PCLs reviewed at multidisciplinary team meetings are intraductal papillary mucinous neoplasms (IPMN), pseudocysts or mucinous cystic neoplasms (MCN). Serous cystic neoplasms (SCN) are less commonly referred due to definitive diagnosis with good cross sectional imaging. Other PCLs including solid pseudopapillary neoplasms (SPN) are far less common.
Serous
Serous cystic neoplasm
Historically termed ‘microcystic adenomas’, these are slowly growing lesions with fibrous structures forming a honeycomb appearance within a well-defined capsule. A central, stellate scar is seen in 30% on CT. About 10%–20% of SCN are oligocystic or macrocystic and can be confused with mucinous cysts. Lobulated contrast enhancement in the cyst capsule may be a clue to differentiating an oligocystic SCN from MCN.5 6
Peak incidence is in the seventh decade of life (75% females). These are most often discovered incidentally, typically in the pancreatic body and tail. Symptoms related to mass effect are occasionally present—anorexia, weight loss, abdominal pain, palpable mass or jaundice.7 8 Lesions are typically unifocal, though multiple cysts may be seen in patients with Von Hippel Lindau Syndrome, 90% of whom have SCN.9 The classic endoscopic ultrasound (EUS) appearance is of a multicystic lesion with small anechoic cysts and intervening hypoechoic areas. Fluid amylase levels and fluid carcinoembryonic antigen (CEA) are not elevated and cyst fluid is not viscous.10 Cytology is often acellular, though may reveal glycogen-rich cuboidal epithelial cells. Fine needle aspirate (FNA) is often bloody.11
The differentiation between serous cystic adenoma (SCA) and serous cystic carcinoma (SCC) is dependent on the demonstration of malignant potential.4 There have been very few reported cases of malignant transformation and surveillance is typically not recommended.12 13 SCNs are not routinely resected.14
Controversy exists around the role for surveillance or surgery when SCAs are diagnosed in younger patients. Indications for resection include suspicion of SCC, significant symptoms and size >4 cm (though size is known to poorly correlate with likelihood of malignancy). Prognosis postresection is excellent, including reports of long-term postoperative survival.15
Solid pseudopapillary neoplasms
SPN are typically large lesions within a fibrous capsule comprised of mixed solid and cystic components. Microscopically, monomorphic epithelial cells form pseudopapillae and haemorrhagic necrosis creates cystic foci. Malignancy is seen in 10%–20%. Lymph node involvement and distant metastases have been reported in cases without features of local invasion.16–18 Molecularly, SPN differs from pancreatic ductal adenocarcinoma (PDAC) by activation of the beta-catenin pathway in most tumours and frequent expression of progesterone receptors.19 Historically SPN present due to mass effect, with symptoms similar to SCNs. Asymptomatic presentations are increasing. More than 80% of SPNs present in females, typically in the fourth decade. Paediatric presentations comprise up to 25% of SPNs.16–18
Cross-sectional imaging reveals a well-demarcated fibrous capsule surrounding a heterogeneous solid-cystic mass. EUS appearance is similar, with a well-defined hypoechoic mass without MPD communication or dilatation. The extent of the solid or cystic components may vary widely. EUS FNA is typically bloody, with low viscosity and low amylase/CEA levels in keeping with a non-mucinous cyst. Cytological features are of pseudopapillary structures and fibrovascular tissue cores with variable eosinophilia.
Surgical resection is favoured due to malignant potential, early median age of diagnosis and symptomatic mass effect.14 Post-resection 5 year survival rates are as high as 95%; however, ongoing surveillance imaging is recommended as the risk of recurrence (10%) extends beyond 5 years.8 20
Mucinous
Mucinous cystic neoplasms
MCNs are solitary lesions, occurring almost universally in the body or tail of pancreas (>97%) of females (>98%) in their fifth and sixth decade of life.21 22 Histologically, these uniloculated or multiloculated cysts are lined by mucin producing duct type epithelium within a fibrous capsule of ovarian type stroma (spindle cells and epithelioid cells). Uniloculated MCNs have been mistaken for pseudocysts and multiloculated lesions may be difficult to differentiate from SCN prior to cyst fluid analysis.8 23
MCNs are, predominately, an asymptomatic finding. The features related to age, gender, solitary nature and location within the pancreas may give strong clues to the diagnosis. Most do not exhibit MPD communication, central scarring is absent and up to 15% contain calcifications of the peripheral capsule.24
MPD communication may be more readily excluded at EUS to differentiate these lesions from branch duct-intraductal papillary mucinous neoplasms (BD-IPMN), though prior endoscopic retrograde pancreatography demonstrating MPD communication has been reported in up to 15% of histologically confirmed MCN.25 MCN is often strongly suspected on clinicoradiological and demographic criteria. EUS is superior to cross-sectional imaging in detecting mural nodules, which along with size >4 cm, is a predictor of malignant behaviour. Fluid analysis typically reveal viscous aspirate with high CEA consistent with a mucinous lesion. Variability in MPD communication likely explains the variation in amylase levels, though this is typically low (a potential point of differentiation with IPMN). Cytology may demonstrate mucinous columnar epithelial cells within background mucin.8 23 26
Cancer is reported in 4%–30% of resected MCNs.23 24 In MCNs without high grade dysplasia (HGD), resection is considered curative. For those with established malignancy at the time of diagnosis, prognosis is much poorer and postresection surveillance is in line with recommendations given for PDAC.23 26 27
Intraductal papillary mucinous neoplasms
IPMNs are mucin producing tumours, which in contrast to other PCNs, characteristically arise in (main duct IPMN; MD-IPMN) or communicate with (BD-IPMN) the MPD. A mucinous cyst in communication with a focally or diffusely ectatic MPD are said to be of mixed type (MT-IPMN) (figure 1). Another point of distinction from other PCNs is that BD-IPMNs are multifocal in 10%–40% of cases.28 29 The invariably dysplastic mucosa of these lesions is analogous in appearance to tubulovillous adenoma of the colon, with columnar epithelium and goblet cells covering prominent papillae (producing copious mucin). There are four epithelial subtypes; gastric (seen in BD-IPMN), intestinal, pancreaticobiliary and oncolytic (latter three seen in MD-IPMN). The Gastric subtype confers the best prognosis and pancreaticobiliary subtype the least favourable.30 It is not routinely possible to determine the epithelial subtype prior to surgery.

Magnetic resonance cholangio-pancreatogram characterisation of intraductal pancreatic mucinous neoplasm: (A) branch duct type, (B) multifocal branch duct type, (C) mixed type, (D) main duct type.
The typical IPMN presents in the sixth or seventh decade of life as an asymptomatic lesion in the head or neck of pancreas (70%). If symptomatic, the classical presentation is of recurrent acute pancreatitis in a patient with a dilated MPD without features of, or risk factors for, chronic pancreatitis.23 28 29 IPMNs are seen on up to 20% of MRI scans visualising the pancreas.31 MD-IPMN can be suspected in patients with focal or diffuse ectasia of the MPD (>5 mm). BD-IPMN are cystic dilatations of pancreatic duct side branches, though MPD communication is not universally appreciable on imaging. If an IPMN is suspected, it can be better characterised by either pancreas protocol CT or gadolinium enhanced MRI pancreas with MRCP.23 30
All IPMN harbour malignant potential. The goal of diagnostic work-up is to determine evidence for MPD involvement or features of invasion as these patients should be considered for resection if they are fit surgical candidates.14 30
EUS is superior to cross-sectional imaging for confirming MPD communication and for the detection of mural nodules as well as for exclusion of alternative diagnoses (eg, pseudocyst or chronic pancreatitis).32 EUS FNA with fluid analysis allows determination of mucinous component as well as cytological analysis which is moderately sensitive, but highly specific for malignancy.33 Further details on assessment, management and surveillance of IPMN follows below.
Approach to diagnostic evaluation of pancreatic cystic neoplasms
Determine the type of cyst.
Scrutinise for current malignant behaviour.
Establish the risk of future malignant transformation.
The clinical context and patient’s fitness for surgery must first be established. Demographics may give clues to the likely aetiology. While 70% of patients will be asymptomatic, symptoms such as pain, weight loss or jaundice should prompt emergent exclusion of invasive disease. Pancreatitis in the context of excess alcohol or gall stones should prompt exclusion of an inflammatory aetiology. Enquiries should also be made into a possible family history of pancreatic adenocarcinoma or genetic syndromes.3 30 34
This review has drawn largely from the The European Study Group on Cystic Tumours of the Pancreas 2018 European evidence-based guidelines on pancreatic cystic neoplasms (ESGCTP guidelines) and the 2017 revised Fukuoka guidelines, both offer current, detailed guidance to clinical practice.3 30 The 2018 American College of Gastroenterology guidelines are broadly in agreement with these.34 The 2015 American Gastroenterology Association guidelines offer less guidance on the management of complex patients, and some of their recommendations have been controversial, such as discontinuing surveillance after 5 years.35
Cross-sectional imaging
Invasive foci in asymptomatic patients with cystic lesions<5 mm in size are rare. Cysts>5 mm should be first evaluated by pancreas protocol CT or MRI. While CT is readily available, MRI gives enhanced resolution of nodules and septae, better delineates duct communication and for these reasons is favoured by recent guidelines3 30 34 (figure 1).
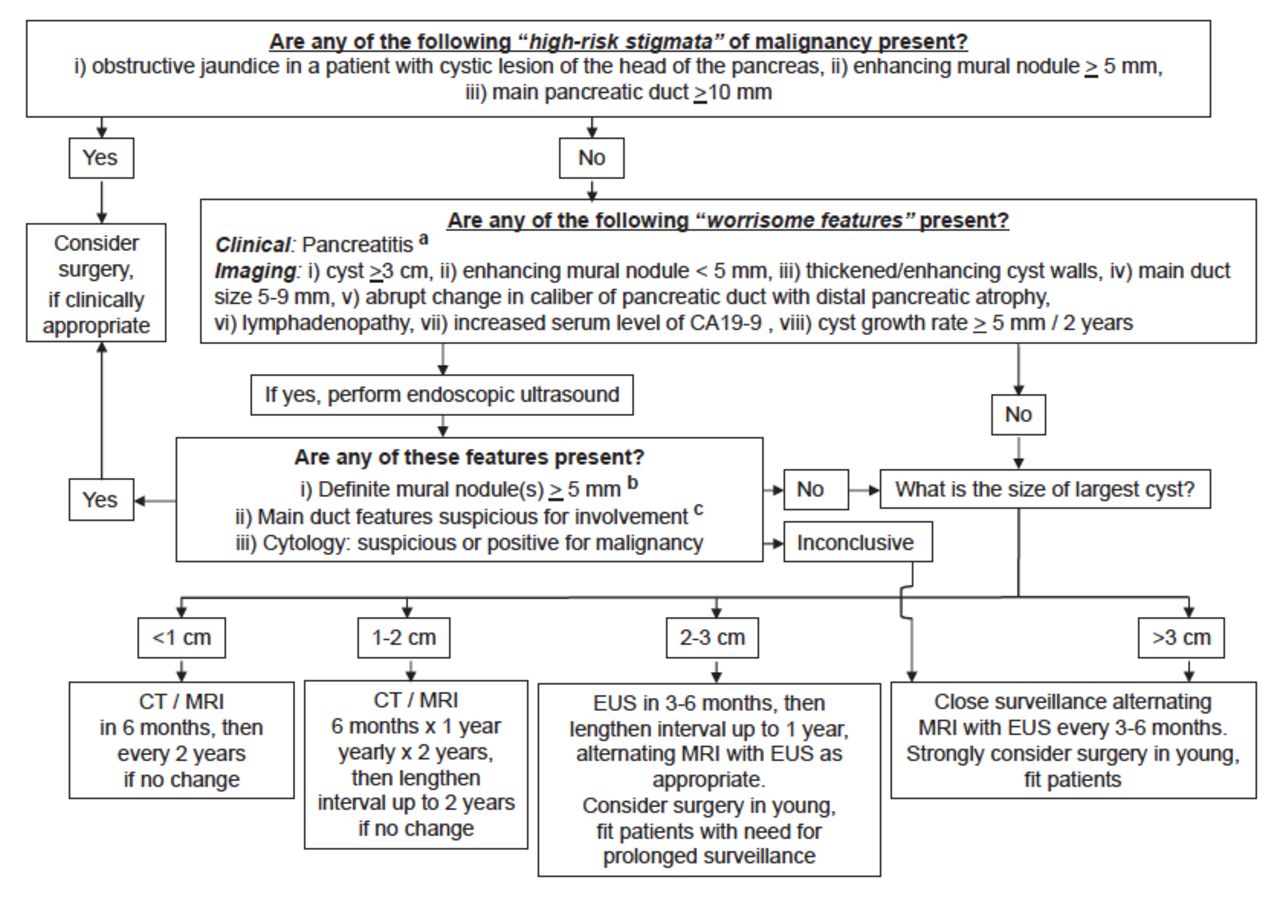
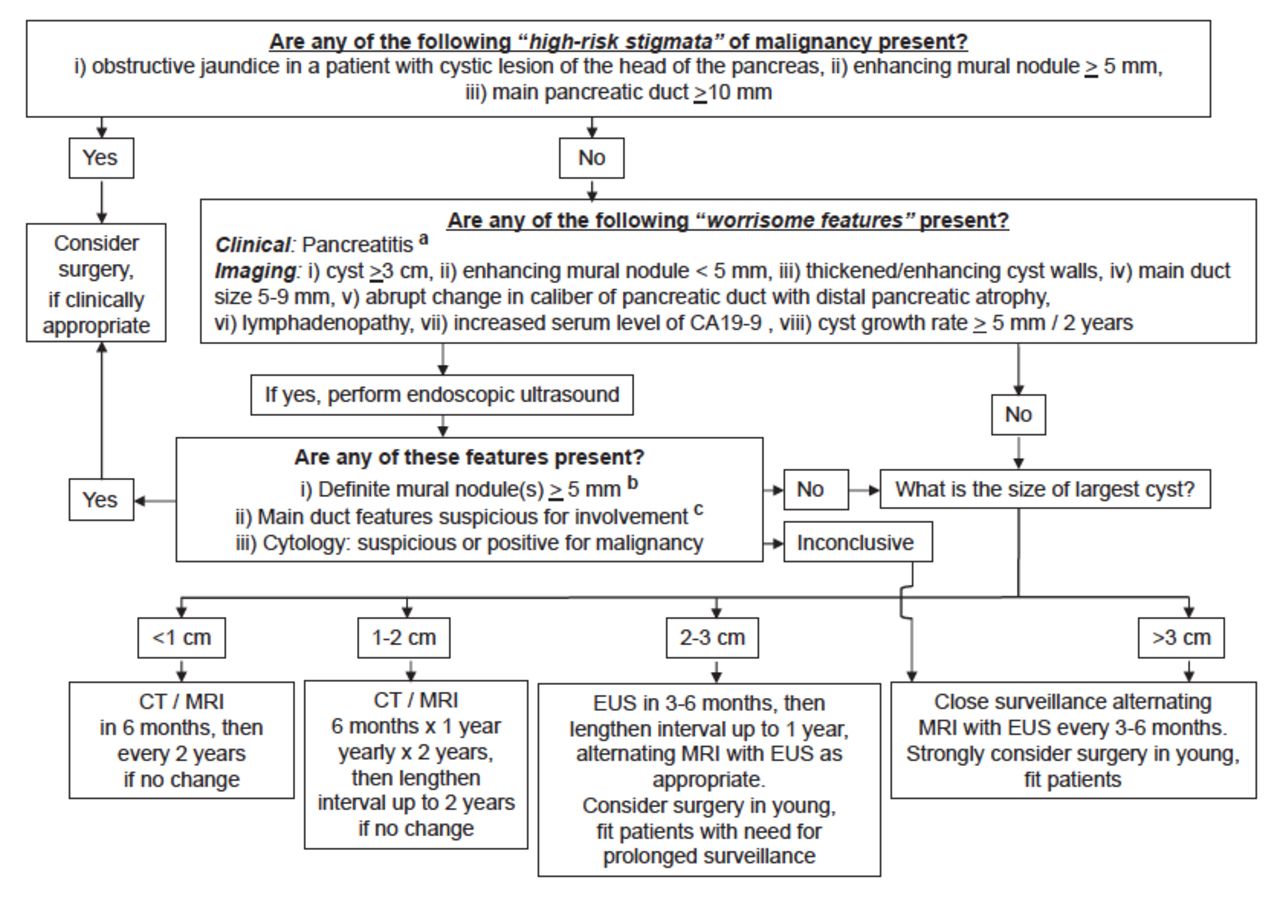
The 2017 revised Fukuoka guidelines outline ‘high risk stigmata’ and ‘worrisome features’ (see table 1). They recommend surgical referral for ‘high risk stigmata’ and EUS assessment for ‘worrisome features’. IPMN 2–3 cm in size without ‘worrisome features’ are advised to have EUS in 3–6 months and smaller cysts to have CT or MRI based surveillance with intervals based on size30 (table 1). The ESGCTP guidelines recommend referral for surgical review for all patients with ‘absolute indications’ and referral based on the consideration of comorbidities and number of risk factors for those with ‘relative indications’ (table 2).3
Risk stratifying characteristics of IPMN used in the Revised Fukuoka Guidelines30
Indications for surgery in IPMN from the 2018 ESGCTP Guidelines3
Positron emission tomography (PET) has utility in detecting distant metastases in the setting of confirmed PDAC preventing unnecessary surgery.36 However, the differentiation of benign from malignant PCN using PET produces variable results.37–40 Using PET for identifying metastatic lesions in patients with high risk features (being considered for surgery) may prove more fruitful.
Endoscopic ultrasound
EUS should be reserved for cases where it is expected to alter management. The high resolution of soft tissue may allow visualisation of septae, nodules, internal debris/mucin and duct communication41 (figure 2). In a retrospective review of 145 cases, EUS demonstrated multifocal IPMN resulting in a change to the surgical field for a significant number of patients compared with both CT (47% vs 13%) and MRI (33% vs 4%). Other trials have not demonstrated an advantage of diagnostic EUS over CT or MRI in the preoperative diagnosis of PCN.42 43 Detection of high risk features at EUS should prompt surgical referral. The 2018 ESGCTP guidelines recommend performing EUS at any point at which a PCN develops clinical or radiology concerns.3
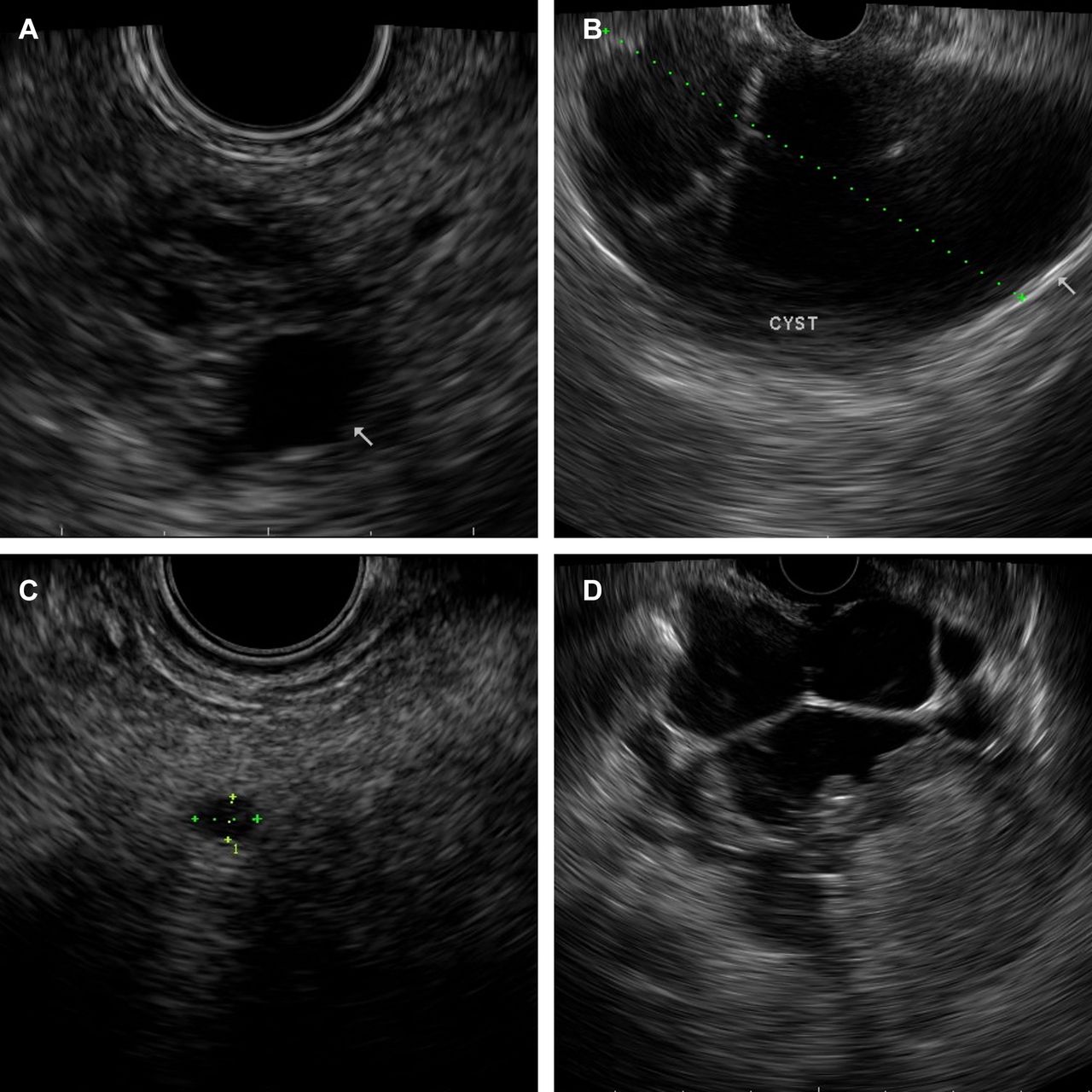
EUS imaging of pancreatic cystic neoplasms: (A) serous cystic neoplasm, (B) mucinous cystic neoplasm, (C) branch duct type intraductal papillary mucinous neoplasm, (D) malignant changes within an intraductal papillary mucinous neoplasm.
Contrast-harmonic enhanced (CHE) EUS can allow demonstration of blood flow to suspected mural nodules, delineating these from mucin and internal debris, as recommended by the 2018 ESGCTP.3
Cyst fluid analysis
An advantage of EUS is the ability to sample cyst fluid. Cyst FNA is invasive and should be performed when expected to alter management, such as IPMN with ‘worrisome features’ or in undifferentiated PCNs. Relative contraindications include the need to traverse >10 mm of pancreatic parenchyma, high-risk bleeding disorders and use of dual antiplatelet therapy.3
A CEA level >192 ng/mL has a sensitivity of 73% and specificity of 84% for the diagnosis of a mucinous lesion.44 Below 5 ng/mL and above 800 ng/mL, the negative and positive predictive values, respectively for mucinous aetiology are both 94%.45 Mucin may be seen on cytological analysis or suggested by a positive ‘string test’.46 Elevated amylase/lipase reflects duct communication, as in IPMN and pseudocysts. Variable amylase/lipase levels seen in MCNs make them an imperfect tool for differentiating mucinous cyst types. The 2018 ESGCTP guidelines advise that the combination of cytology, CEA and lipase provides the highest diagnostic accuracy in differentiating mucinous from non-mucinous PCN.3
Low cellularity hampers cytological detection of malignancy and differentiation of PCN type. The sensitivity for detecting HGD and carcinoma in IPMN is only 50%, though as high as 72% if limited to use in cysts with worrisome features.30 Its strength is in its specificity—suspicious or malignant cytology should prompt surgical referral.
Despite these limitations, EUS FNA reduces inappropriate surgery for asymptomatic serous lesions and inappropriate surveillance of high-risk lesions under 3 cm in size.47 Doing so alters management in 36% of patients evaluated by CT and 54% of those evaluated by MRI.48
Other adjuncts to endoscopic evaluation of pancreatic cystic neoplasms
A pouting, ‘fish-mouth’, major ampulla, with appreciably mucoid secretions is indicative of main duct involvement by IPMN. This is best seen with a side-viewing duodenoscope.30
Pancreatoscopy allows visualisation of the papillary projections of MD-IPMN and MT-IPMN facilitating directed biopsy, distinction from other causes of dilated MPD and determination of the extent of MPD involvement preoperatively.49
The endoscopic evaluation of PCNs is not dependent on any one diagnostic feature, but rather relies on the synthesis of information from the EUS imaging, cytology, cyst fluid analysis and any diagnostic adjuncts. This was eloquently demonstrated by Oppong and colleagues who showed that a combination EUS diagnosis (endosonographic impression, cytology and CEA level) had a sensitivity (91%), specificity (75%) and accuracy (85.7%) higher than any test component in isolation (p<0.05, for all comparisons).50
Approach to management
A major hindrance in the management of PCN relates to establishing a histological diagnosis in cysts which are not resected. Cysts with an uncertain diagnosis should be managed as per mucinous cysts.3
Surgical resection
While universal resection of MCN had been recommended,26 there is a paucity of evidence for this approach.35 ESGCTP guidelines recommend resection of MCN≥40 mm, if symptomatic or if harbouring risk factors such as mural nodules.3 These lesions are typically found in the distal pancreas of younger patients and may be amendable to less morbid distal pancreatectomy.
Most guidelines consider MD-IPMN and BD-IPMN separately, based on mean rates of HGD or invasive disease, of 62% in MD-IPMN. The 2017 revised Fukuoka guidelines quote 5-year survival rates for resected MD-IPMN far superior to PDAC (31%–54%) and recommend resection of MD-IPMN in surgically fit patients with MPD >10 mm, jaundice or mural nodules.30 The 2018 ESGCTP guidelines go further. While similarly including MPD>10 mm as an ‘absolute indication’ for surgery, they consider MPD of 5–9.9 mm as a ‘relative indication’, citing published rates of HGD or cancer of 37%–91% (vs 56%–89% in MPD >10 mm).3 In diffusely dilated MPD, efforts should be made to establish the extent of duct involvement. This can determine the suitability for segmental resection and ensure these criteria are not mistakenly applied to other causes of MPD dilatation (eg, chronic pancreatitis). This could be established preoperatively with intraductal ultrasound or pancreatoscopy or by intraoperative frozen section.49 54 55
A considerable number of BD-IPMN harbour HGD or invasive carcinoma (14%–48%) at diagnosis and should be resected.56–59 The remainder have a low annualised rate of malignant progression (1%–7%) lending themselves to surveillance.60–62 The 2017 Fukuoka guidelines indications for surgery from cross-sectional imaging are described in table 1. EUS criteria prompting surgical referral are then mural nodule ≥5 mm, MPD involvement and cytology suspicious or positive for malignancy.30 The 2018 ESGCTP list similar ‘absolute indications’ for surgery (table 2). Their relative indications (table 2) include biochemical, cyst and clinical features to be considered on the balance of patient comorbidities.3 In both guidelines, patients not meeting these criteria enter surveillance as described below.
Multifocal disease, present in 14%–41% of BD-IPMN, should be considered when planning the type of resection.63–65 The physiological function of residual pancreas must be taken into account. The ESGCTP recommend resection only of those cysts exhibiting indications for resection, with per protocol surveillance of unresected cysts.3
Surveillance
After consideration of the ‘high-risk stigmata’ and ‘worrisome criteria’, the 2017 revised Fukuoka guidelines stratifies patients by cyst size. EUS is indicated both in cysts>3 cm (alternating every 3–6 months with MRI) and in cysts 2–3 cm (EUS within 3–6 months of detection and then annual surveillance alternating EUS and MRI). Cysts of 1–2 cm are monitored by CT/MR 6 monthly for 1 year, annually for 2 years, then biannually if no changes detected, while those <1 cm are reassessed at 6 months before biannual surveillance with CT/MR. Any concerning evolution not meeting the criteria for surgery should prompt shortening of surveillance interval (3–9 months) (figure 3).30
{kind=link}
{kind=link}
{kind=link}
The 2018 ESGCTP guidelines recommend clinical and radiological (MRI and/or EUS) follow-up 6-monthly in the first year, then annually, for both IPMN and MCN. For IPMN they advise serum CA19.9 at each of these time points.3
The 2017 revised Fukuoka guidelines highlights the not infrequent development of both new IPMN and concurrent PDAC lesions, regardless of the presence of HGD at resection, with reports of this occurring beyond 10 years postresection.30 They reference a 10-year IPMN recurrence rate of 62% with invasive IPMN in 38%.66 67 They recommend at least twice yearly surveillance with cross-sectional imaging in high risk patients (family history of PDAC, HGD at resection margin and non-intestinal IPMN subtype) and 6–12 monthly surveillance in others for as long as they remain candidates for surgical resection.30 The 2018 ESGCTP guidelines recommend surveillance as long as the patient remains fit for surgery. Any patients with foci of carcinoma are followed as per PDAC, patients with HGD or MPD involvement should be followed 6-monthly for 2 years and then annually, while all others should be followed as per unresected cysts.3
Can we stop surveying?
The 2015 AGA guidelines aside, all other guidelines recommend continuation of surveillance of all unresected IPMN for as long as the patient remains fit for surgery.3 30 34
Future directions
A recent study by Krishna and colleagues investigating intracystic needle confocal laser endomicroscopy demonstrated sensitivities, specificities and diagnostic accuracies≥94% for mucinous cysts and ≥98% for SCAs. Intraobserver reliability and inter-observer agreement were near perfect for mucinous cysts and SCAs (kappa values>0.80).68 Recently published guidelines advised awaiting large prospective studies before this technique is recommended outside research settings.3 Microbiopsy forceps deployed via a 19 gauge FNA needle may improve sample cellularity, though robust data does not yet exist.31
There has been much interest in the development of DNA and molecular markers to improve cyst fluid analysis. K-ras proto-oncogene mutations strongly correlate with mucinous cysts, and their concurrence with aneuploidy or allelic loss is 96% specific for malignancy.69 70 Guanine nucleotide binding protein mutations may have potential in differentiation of highest risk mucinous cysts from the more indolent.71 Neither are widely available. The 2018 ESGCTP guidelines advise that both can improve the detection of malignant change in mucinous cysts. There have been positive results using mass spectrometry of peptides such as mucin-5AC and mucin-2 to detect high risk mucinous cysts, though these findings require further validation.72
Interest exists in minimally invasive therapies to halt malignant progression of mucinous cysts. Ablative therapies investigated include intracystic injection of ethanol and/or paclitaxel and radiofrequency ablation using a needle-based probe. These therapies remain investigative and should only be considered in non-operative candidates in trial settings.73
Key points from this review
Pancreatic cystic lesions are common and accurate diagnosis can be difficult.
The synthesis of clinical, radiological, biochemical and histopathological information needs to be prioritised over any single investigation.
Correct differentiation between high-risk and low-risk PCN is important to guide appropriate allocation to surgery, surveillance or reassurance.
Surgical options should be defined by location of lesion, patient factors and the malignant risk of the lesion. Mucinous cysts, in fit lesions, not meeting criteria for resection are surveilled.
Further research is required to inform diagnostic, treatment and surveillance algorithms.
References
Footnotes
Contributors Research, tables and manuscript draft: MJK. Contribution to manuscript revisions and figures: MJK and BP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.