Article Text

Abstract
Anorexia nervosa (AN) is a complex eating disorder associated with a high morbidity and mortality, however, there is a lack of dedicated training for healthcare professionals outside of mental health specialities. There has been a reported increase in acute admissions of patients with AN, which may have been precipitated by the isolation and loss of support networks created by the COVID-19 pandemic. The purpose of this review is to highlight that AN can present with a wide variety of signs and symptoms relating to both the hollow and solid organs of the gastrointestinal (GI) tract some of which may even be life threatening. The overlap of symptoms with several other functional and organic GI diseases makes diagnosis challenging. Gastroenterologists and allied healthcare professionals need to be aware of the wide array of possible GI manifestations not only to help rationalise investigations but to also facilitate early involvement of the relevant multidisciplinary teams. Many of the GI manifestations of AN can be reversed with careful nutritional therapy under the guidance of nutrition support teams.
- nutrition
- motility disorders
- liver
- pancreas
Statistics from Altmetric.com
Introduction
Although the precise prevalence of anorexia nervosa (AN) remains elusive, a recent systematic review reported a lifetime prevalence of 1.4% in women and 0.2% in men.1 AN has the highest mortality of all psychiatric illnesses, and medical complications are said to account for more than half of these deaths.2 AN is characterised by: persistent pattern of behaviours aimed at creating a calorie deficit leading to significantly low body weight which is overvalued or inaccurately perceived as normal.3 There are two subtypes of AN: restrictive subtype (AN-R) and binge-purge subtype (AN-BP) characterised by binge eating followed by self-induced vomiting, laxative or enema abuse.3 Despite the subtype of AN which includes bingeing and purging, the diagnosis differs from bulimia nervosa (BN) as demonstrated in table 1.3
ICD-11 comparison of anorexia nervosa (AN) and bulimia nervosa (BN) essential criteria3
A 2012 high profile case of one teenager’s avoidable death due to the complications of AN, triggered a UK parliamentary ombudsman investigation and the publication of a report in 2017 entitled: ‘ignoring the Alarms: How NHS eating disorder services are failing patients’. The report highlighted several failings in the care of this group of patients including within the acute hospital setting and called for better training in the recognition and management of eating disorders as a whole.4 This comes as little surprise given that a UK-wide survey of medical schools identified less than 2 hours of teaching was being dedicated to eating disorders.5 This study also highlighted the paucity of postgraduate training with the majority of trainees receiving no dedicated education or training, with the exception of child and adolescent psychiatry trainees.5 This is compounded by a global lack of nutrition education for medical students, which was identified by a systematic review, with demonstrable impact on knowledge and confidence.6
Over the last year, an increased number of AN admissions has been recognised, in one setting over 100% increase has been reported.7 Whether this is related to the destabilisation of eating and exercise habits created by the COVID-19 pandemic and the subsequent lockdowns or whether this growth will continue beyond the pandemic remains to be seen. A recent UK survey conducted early in the pandemic identified that those with current or past eating disorders were adversely impacted and had perceived increased preoccupation with food, exercise and appearance.8
Although the majority of the evidence is limited to case reports and case series gastroenterologists are positioned to identify the gastrointestinal (GI) physical manifestations of AN and involve the relevant multidisciplinary team early (table 2 and figure 1). A survey of predominantly patients with AN identified 62% had reported a GI symptom to either a gastroenterologist or primary care doctor.9 Interestingly of these 46% had sought help for their GI symptoms first and 38% underwent some form of GI investigation which included endoscopy.9 Studies have also reported an association between AN and chronic GI illnesses such as Crohn’s disease and coeliac disease.10 11
{kind=link}
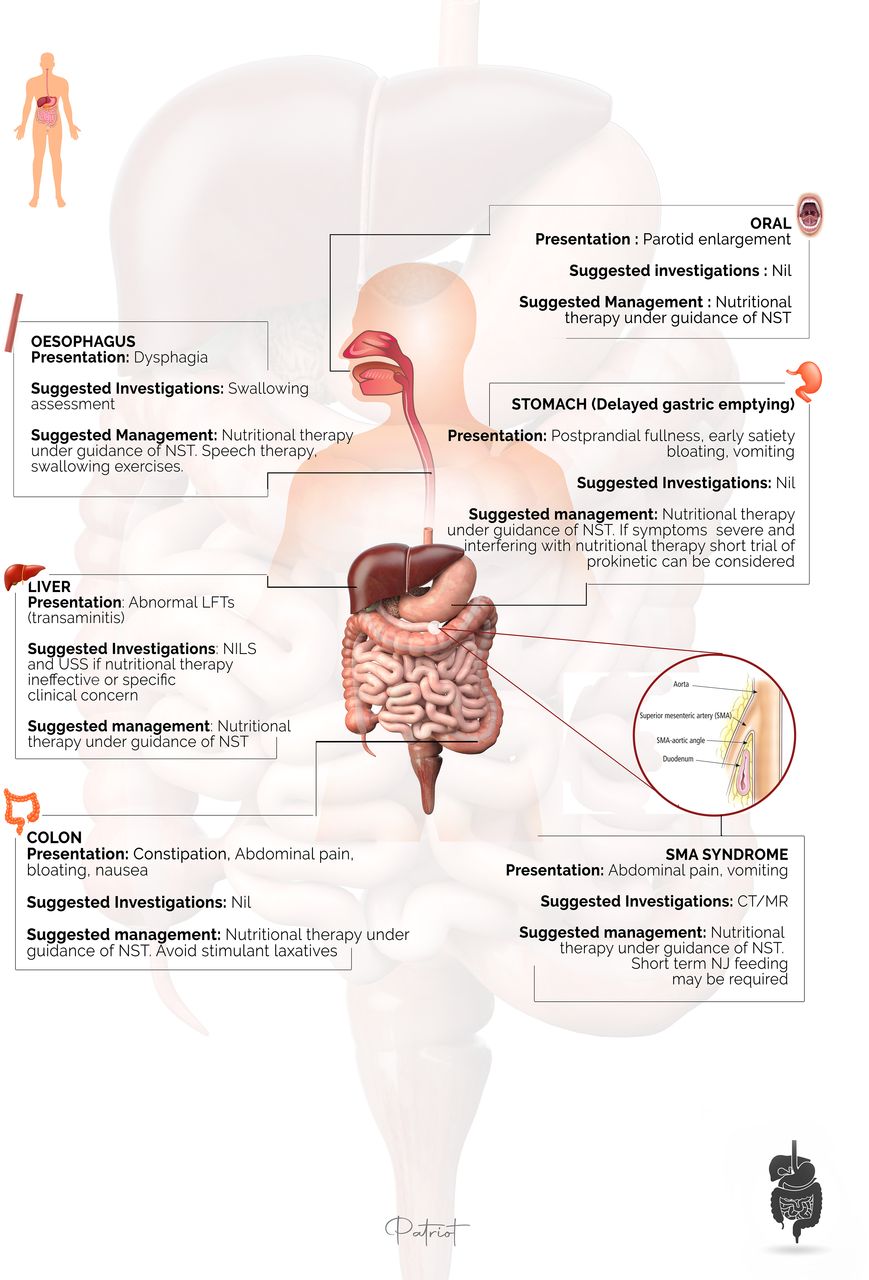
Gastrointestinal manifestations of AN. CT, computed tomography; LFT, liver function test; MR, magnetic resonance; NILS, non-invasive liver screen; NJ, nasojejunal; NST, nutrition support team; SMA, superior mesenteric artery; USS, ultrasound scan.
A summary of the GI manifestations of anorexia nervosa
We appreciate that AN is a complex condition with many considerations beyond the GI physical manifestations which include genetic, environmental, neurological, psychiatric and psychological but are beyond the scope of this review. An additional tier of complexity also revolves around recognising that GI symptoms may also be caused or exacerbated by:
Caffeine
Diet pills
Herbal remedies
Laxatives
Substance use including (but not exclusive to) alcohol and cannabis
Sweeteners (sorbitol)12 13
Upper GI tract
While rare and limited to case reports, AN can mimic both GI and non-GI disorders. There are several case reports in the literature of alternative diagnoses being initially mistaken for AN such as:
Achalasia
Astrocytoma of the medulla
Choroid plexus papilloma
Chronic giardiasis
Coeliac disease
Crohn’s disease
Oesophageal spasm
Upper oesophageal sphincter hypertonicity10 14–18
On the other hand GI symptoms in AN can be difficult to separate from functional bowel disorders and in one study using the Rome II modular questionnaire they identified 55.6% of patients with AN reported symptoms of irritable bowel syndrome; 42.2% functional heartburn and 31.1% functional abdominal pain and 42.2% had at least three coexistent functional GI disorders.19
Oral
As with many areas of physical health in patients with AN, there is limited data and due to the nature of the condition studies tend to include both paediatric and adult populations. One study, assessing dental health in AN, BN and controls, demonstrated patients with AN had higher levels of plaque, gingivitis and gingival recession and reported brushing their teeth more frequently than any other group.20 The reason for this is theorised to be that increased brushing is a distraction technique to avoid eating and as a consequence causes traumatic gingival recession.20 Studies in patients with AN have also demonstrated an impact on parotid size and function with one of these studies demonstrating a reduction in parotid flow rate, quantity and quality of saliva.21 Parotid enlargement and hyperamylasaemia can be encountered by gastroenterologists and although less common than in BN, it has been reported in AN of both subtypes.22 23
Oesophago-gastric
Upper GI symptoms are commonly reported in AN and can cause significant management challenges. Studies have identified postprandial fullness, early satiety, nausea, vomiting, heartburn, abdominal distention and pain as frequently reported symptoms.24–26 There are multiple case reports, case series and small studies which have shown upper GI abnormalities including oropharyngeal dysphagia (OPD), increased lower oesophageal sphincter pressure and delayed gastric emptying.15 27–29 Loss of intra-abdominal fat may also precipitate a superior mesenteric artery syndrome, leading to abdominal pain and vomiting.2
Although a rare complication, it has been postulated that decreased gastric motility and emptying in AN can predispose to acute gastric dilatation after bingeing which, if unrecognised, can lead to necrosis and even rupture.30 31 In Benini et al’s study, although patient numbers were small, they observed that as AN symptoms improved there was a normalisation of lower oesophageal sphincter pressure but upper GI symptoms did persist.28 One study demonstrated that those with AN who presented with OPD (found more often in the AN-R subtype) had a lower body mass index (BMI) (mean 12.0±1.9 kg/m²).27 In this study, of those patients with AN with OPD who went on to have video fluoroscopy, this was abnormal in over 70% and the authors postulated that diminished muscle tone was the underlying pathology.27 There is a small case series which supports this hypothesis and demonstrated improvement, but not normalisation, of dysphagia with neuromuscular electrical stimulation alongside speech and language therapy but long-term and prospective studies are lacking.29
Many of the studies demonstrated that reinstitution of feeding can improve gastric emptying without pharmacological therapies, although patient numbers were small. An example of this would be the study by Rigaud et al,which confirmed this finding in 11 of 14 patients who gained weight during the study period.32 Improvement in GI symptoms following the reintroduction of oral nutrition was also demonstrated in one study of 16 patients with AN.33 This was achieved by gradual titration of 500 calories per week over an average twelve week period and demonstrated that patients with AN could also tolerate calorie regimes of up to 4500 per day.33 Prokinetics such as domperidone, metoclopramide and erythromycin have been shown to have a positive effect on gastric emptying in AN and could be considered on a short-term basis if symptoms hinder the tolerability of nutritional therapy but potential side effects need to be carefully weighed up.15 34 35 QT interval needs to be considered before embarking on any prokinetic therapy as patients with AN may be on other QT prolonging drugs (antidepressants/antipsychotics) and may have electrolyte (hypokalaemia/hypomagnesaemia) and structural cardiac abnormalities.36 Pragmatically, once the refeeding risk period is over, metoclopramide could be considered as a possible first line prokinetic on a short term and case-by-case basis.
There is some evidence for a potential association between AN and oesophageal squamous cell cancer possibly, in some, as a result of smoking (higher prevalence of smoking in AN-BP subtype) and alcohol consumption being exacerbated by chronic malnutrition.37–39 While a later meta-analysis appears to suggest that those with AN were not found overall to be significantly more likely to be lifetime smokers than healthy controls (the opposite being true for those with BN) the authors highlight that sub-group analysis of the AN-BP subtype was not possible.40 They discuss that the impulsivity similarities between the AN-BP subtype and BN might explain a higher prevalence of smoking in AN-BP which they were unable to detect based on the way their included studies reported data.40 One study assessing 3617 patients found a sixfold increase in oesophageal squamous cell carcinoma with seven patients, aged between 35 and 72, diagnosed between 19 and 28 years after diagnosis of AN.37 More prospective cohort studies are required to explore these possible associations further.
Liver
Liver enzyme abnormalities are common in AN: mild to moderate elevations in aminotransferases have been, reported in several studies, with alanine aminotransferase (ALT) being disproportionately more elevated than aspartate aminotransferase (AST).41 42 As liver injury progresses and glycogen stores are depleted, hypoglycaemia becomes a significant concern and serves as a poor prognostic indicator.43 A retrospective study of 181 (65.8% AN-R) patients admitted for medical stabilisation reported mild elevations in AST or ALT in 27.6% and severe elevations (greater than three times upper limit of normal) in 35.4%.44 This study identified that those with severely elevated liver enzymes on admission had a median BMI of 11.9 kg/m²±1.8 kg/m².44 Following a period of nutritional replenishment the majority of patients had normalisation of their AST and improvement in their ALT at the point of discharge.44 This study also identified that those with severely elevated liver enzymes were more likely to be AN-R subtype, had an increased risk of developing severe hypoglycaemia and were more likely to have a prolonged length of stay.44 An elevated ALT during the refeeding period has also been shown to significantly associated with a delay to the start of weight gain.45 Another study (57% AN-R subtype) also reported a BMI threshold of 12 kg/m² as a significant risk factor for elevated liver enzymes.42 This retrospective study of 126 patients identified age below 30, male sex and AN-R as other risk factors for liver enzyme elevation in univariate analysis however only BMI remained significant in the multivariate analysis.42 Following 4 weeks of careful but progressive inpatient enteral nutrition the majority of patients had a resolution of their transaminitis.42 It is therefore generally accepted that the greater the degree of malnutrition, the worse the liver enzyme abnormalities.41 42 Rarely, patients can present with an acute hepatitis with aminotransferases running into the thousands and this has been reported in two case reports.46 47 In both of these cases a standard non-invasive liver screen and imaging did not identify any other obvious cause and liver function tests improved significantly with nutritional therapy.46 47
Many mechanisms have been highlighted as a possible explanation for abnormal liver biochemistry in patents with AN. This includes ischaemic hepatitis from hypoperfusion and steatosis which develops during refeeding.48–50 Another postulated mechanism for abnormal liver biochemistry is autophagy; the cellular process in which old cytosolic proteins and organelles are degraded with the resultant recycling of the breakdown products for cellular use.51 Rautou et al performed liver biopsies in 12 patients with AN presenting with acute liver insufficiency who had a median BMI of 11.3 kg/m² and no other identifiable cause for liver disease.52 Liver biopsies showed autophagosomes in four patients: a hallmark of autophagy.52 Autophagy in a patient with severe malnutrition is initially postulated to have a protective effect by recycling nutrients and preventing cell death.52 Progression of malnutrition can cause this process to become excessive, and no longer protective, leading to cell death and acute liver failure.51 52
In summary, secondary causes of elevated liver enzymes are not usually found and the mainstay of therapy is nutritional repletion which should be under the guidance of a nutrition support team (NST). Awareness of this may limit the need for more invasive investigation into the cause of abnormal liver biochemistry in patients with AN.
Pancreas
Thirty per cent of cases of acute pancreatitis are labelled as idiopathic.53 AN, however, is overlooked as a possible cause within this idiopathic group, however, the evidence in the literature is limited to case reports and case series (table 3). There is often an overlap of symptoms in AN and pancreatitis, not exclusive to, but including: vomiting, abdominal pain and elevated amylase. It should be noted that elevated amylase can be the result of purging and release from the salivary glands.54 Such a rise should be evaluated within the clinical context because, in isolation, it does not necessarily point towards a diagnosis of pancreatitis.54
Summary of case reports of pancreatitis in AN
There have been several speculative mechanisms put forward as possible explanations for acute pancreatitis in AN. One of these proposed mechanisms is that starvation and dehydration results in thickened pancreatic secretions clogging pancreatic ducts and a sudden increase in calorie intake stimulates the pancreas against this high pressure backdrop resulting in acinar rupture.55 Another mechanism is hypoperfusion as a result of severe dehydration and hypotension which can result in multiorgan damage which includes the pancreas. This was proposed as an explanation for a lipase and amylase of 1437 and 1002, respectively, in one particular case report of a female patient with AN who had weight loss to 24.5 kg (BMI 10.8 kg/m2).50
In severely malnourished patients, it has been postulated that the loss of the fat pad around the superior mesenteric artery results in compression of the duodenum between the aorta and the vertebral column posteriorly, resulting in a duodenal ileus and high pancreatic duct pressures.55 56 Refeeding may compound this and there are several reports of pancreatitis developing following the introduction of enteral nutrition in both the paediatric and adult literature.57 58
In some of the case reports highlighted in table 3, clinical symptoms, pancreatic enzyme levels (<3 times upper limit of normal in some cases) and imaging findings would not necessarily fulfil modern standard definitions for acute pancreatitis and described abnormalities may be secondary to other causes.59 If pancreatitis is suspected in patients with AN, broad (often related) causes should be considered. One previous study demonstrated fat intake of less than 10 grams resulted in reduced gallbladder emptying and therefore increased biliary stasis, a known risk factor for gallstone formation.60 Further investigations should be considered if pancreatitis is suspected, including intra-abdominal imaging and more specific pancreatic enzymes (lipase or amylase isoenzyme).
Small bowel and the colon
Evidence has been emerging relating to links made between the intestinal microbiome and the impact this may have outside of the alimentary tract, such as satiety, mood or behaviour (microbiota–gut–brain axis). This could potentially exacerbate conditions such as AN.61 62 One study demonstrated dysbiosis (significantly lower diversity) in AN and this was associated with greater anxiety and depression.63 A study performed by Mack et al demonstrated an increase in diversity with nutritional repletion and weight gain without improvement in GI symptoms.64 Several studies in patients with AN have reported dysbiosis in the abundance and diversity of gut microbiota although the differences are not consistent and sometimes contradictory (eg, Firmicutes/Bacteroidetes ratio).63–65 The microbiota can also vary between AN-R and AN-BP subtypes and in one study clostridium difficile was isolated only in patients with AN-BP subtype, which was felt to be secondary to behaviours (recurrent purging was postulated as a risk factor for clostridium difficile colonisation) as none of the participants had taken antibiotics and only one was on a proton pump inhibitor.66 Although there is a dearth of human studies, bacterial metabolites such as short-chain fatty acids (SCFA) have been postulated as potential mediators for psychological functioning and is an area of growing interest.67 Understanding how SCFA influence the gut–brain axis and its influence on appetite, behaviour and mood may lead to new therapies and one study in patients with AN demonstrated that reduced faecal butyrate levels were associated with increased anxiety and depression scores.65 It is not currently possible to make any generalisations from microbiota studies in AN as the results are inconsistent which may be related to differences in study designs, statistical analysis, diet variations and severity of AN. There are several other microbial metabolites such as norepinephrine, dopamine and serotonin that may also influence disease course in AN but more studies are required to understand the impact on gut–brain interaction.68 Studies in mice who received microbiota from AN-R patients demonstrated a reduction in body weight gain and food intake suggesting a link to AN-specific dysbiosis.69 A case report of faecal microbiota transplantation (FMT) in a patient with AN reported overall improvement in bacterial diversity but this did not translate into improved clinical outcomes including GI symptoms, mood, behaviour or weight.70 More studies in humans are required to establish whether FMT has a role.70
The difference in whole gut transit time between patients with AN and healthy individuals has been studied.71 72 These studies used lactulose breath testing to demonstrate prolonged mouth-to-caecum transit times in 2 cohorts of patients with AN. Kamal et al compared nine patients with AN to nine controls (mean 109±33.5 min vs 84±27.7 min) and Hirakawa et al compared 9 patients with AN with 10 controls (mean 117±31 min vs 81 min ±33 min). These differences were independent of medication with anticholinergic properties in Kamal et al’s study.71 While the marked variability in transit time meant this did not reach clinical significance in Kamal et al’s study, clinical significance was demonstrated by Hirakawa et al 71 72
In much the same way as gastric motility, there is a significant body of evidence to suggest a link between AN and colonic motility with constipation being commonly reported in patients with AN.33 71 Conversely, disordered eating was reported in 19% of patients presenting to a tertiary centre with chronic constipation.73 Two small studies (totalling 25 patients with AN) showed that colonic transit returned to normal in the majority within 4 weeks of commencing a calorie feeding regimen.74 75 Chiarioni et al noted the presence of pelvic floor dysfunction in 5 of 12 patients which did not improve with treatment and so obstructive defecation syndrome should be considered if symptoms persist despite evidence of improved colonic transit.74 Vigilance needs to be adopted in the treatment of constipation in this cohort as up to 60% misuse laxatives.76 The degree of constipation can be severe with a case report describing fatal necrotising colitis felt to be secondary to faecal obstruction in a patient with AN.77 There are several case reports of bowel ischaemia and necrosis involving both the small and large bowel presenting either insidiously or acutely in AN with mortality as high as 80%.78 79 Although the mechanisms are poorly understood it is believed a non-occlusive compromise to the blood supply in a severely malnourished patient with gut paralysis, gut distention and faecal impaction all play a role, with several of the cases reporting prior binge type behaviour or refeeding as precipitating factors.78 79
Summary of alimentary tract manifestations of AN
It is unclear whether the reported increase in acute admissions due to AN will be persistent although it highlights the importance of an increased awareness of the wide array of GI manifestations. This vigilance may help rationalise investigations and facilitate an earlier referral to a psychiatrist and/or psychologist. There is a significant burden of functional GI symptoms, GI signs and abnormal biochemistry in AN with a tendency to improve with adequate nutrition. Reintroduction of feeding requires careful consideration and avoiding sudden and large increases in calories in those severely malnourished may prevent complications such as, pancreatitis, ischaemia and poor tolerance. AN can be challenging to manage and we would therefore advocate the early involvement of an NST.
Care does need to be taken to exclude organic pathology if symptoms or clinical suspicion persists despite adequate nutrition or weight normalisation. It is also important to be aware of rare but potentially fatal conditions such as acute gastric dilatation and bowel ischaemia with necrosis especially given symptoms can also present insidiously.
Pharmacotherapy is not usually core to the management of the GI manifestations of AN but can be considered on a case-by-case basis. If felt appropriate, osmotic laxatives are preferred and stimulant laxatives avoided. Prokinetics should only be trialled after a period of stabilisation following refeeding and for as short a time as possible
Larger randomised controlled trials are lacking, and further research is needed although there appears to be some promising research into the role of the microbiota and its influence on the gut–brain axis, which may lead to changes in future management. When managing a patient with AN, one of the challenges facing gastroenterologists is to provide optimal care to a cohort who are in a high stress state who can be resistant to therapeutic intervention. The importance of adopting a holistic approach cannot, therefore, be overstated. There is real need not only to increase awareness but to also improve knowledge, skills and confidence by introducing more content on AN into undergraduate and postgraduate curricula of all healthcare professionals involved in the care of these complex patients.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @GastroNW
Contributors WJ submitted the article.WJ and JM wrote, planned and edited the manuscript.WJ and JM both take responsibility for the overall content
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- UpFront