Article Text

Abstract
Introduction Patients with suspected pancreaticobiliary cancers frequently undergo endoscopic retrograde cholangiopancreatography (ERCP) to obtain brush cytology for confirmatory diagnosis. The outcome of this often leads to the management of the patient and can avoid more invasive investigations. There is a wide range of sensitivities and specificities reported in the literature.
Aims To determine the accuracy of the brush cytology obtained at ERCP by performing a retrospective audit of all patients admitted to Guy's and St. Thomas’ Hospital for ERCP during 2008–2013. Also, to evaluate the impact of cytology results on patient care following ERCP.
Method Data were collected from 4 January 2008 to 27 December 2013. This involved analysing EndoSoft (the in-house software for endoscopic data entry), Pathnet (the pathology database) and Electronic Patient Records.
Results 162 patients underwent brush cytology during ERCP. 58 patients had positive cytology. With intention-to-treat analysis, sensitivity was 54.7%, specificity was 100.0% and negative predictive value was 53.9% with a positive predictive value of 100%. Patients with a positive brush cytology result required fewer investigations compared with patients with a negative cytology result.
Conclusions Our results compare favourably with previous studies in the field. Brush cytology has been ignored in recent times due to perceived poor results and efficacy. Our audit shows that it can reduce the number of investigations required to reach a diagnosis of malignancy and so is a valuable tool in the diagnosis of pancreaticobiliary malignancies. However, better guidance on preparation of samples for cytology is needed to reduce the number of insufficient samples.
- BILIARY ENDOSCOPY
- BILIARY OBSTRUCTION
- BILIARY STRICTURES
- ENDOSCOPIC PROCEDURES
- ENDOSCOPIC RETROGRADE PANCREATOGRAPHY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- BILIARY ENDOSCOPY
- BILIARY OBSTRUCTION
- BILIARY STRICTURES
- ENDOSCOPIC PROCEDURES
- ENDOSCOPIC RETROGRADE PANCREATOGRAPHY
Introduction
On average, 48 000 endoscopic retrograde cholangiopancreatography (ERCP) procedures are performed each year nationally.1 They are valuable in the diagnosis and management of pancreaticobiliary strictures as they can obtain tissue for histopathological/cytopathological diagnosis, establish the site and cause of obstruction and deliver therapeutic treatments.2 Brush cytology, in particular, is used frequently with ERCP to help diagnose pancreaticobiliary malignancy as it is a simple, safe procedure that allows sampling from various sites within the biliary and pancreatic tracts.3 However, over the years sensitivities ranging from 6% to 64% have been reported in the literature.4 In some of these prospective studies, extra resources were allocated to the obtaining and processing of cytology samples, such as the presence of a cytologist or a technician to review and prepare samples, and it has been suggested that high yields of brush cytology cannot be obtained in everyday clinical practice. However, we emphasise that our audit is a retrospective analysis of a routine cytology service, in which samples were prepared by endoscopy assistants. The low sensitivities in several previous studies, combined with the availability of more recent diagnostic procedures such as magnetic resonance cholangiopancreatography (MRCP) and endoscopic ultrasound (EUS), have led to questions over the utility of ERCP brush cytology in diagnosing pancreaticobiliary malignancy. Low sensitivity is attributed both to the technical difficulty experienced in obtaining an adequate cellular yield from the stricture and to the very small size and well-differentiated nature of the tumours that make cytological interpretation difficult.5 Additionally, the risk of complications from ERCP can vary between 4% and 30%.6–10
So despite its wide usage, ERCP remains a procedure whose diagnostic value is challenged and the greater availability of MRCP and EUS has resulted in ERCP becoming almost exclusively a therapeutic procedure.11 However, it continues to be the bridge between radiological imaging and surgical intervention in most cases where pancreaticobiliary malignancy is suspected. Due to its relative ease and safety, many studies have suggested that cytology during ERCP, despite its low sensitivity, remains effective for the diagnosis of biliary strictures.12–15 The British Society of Gastroenterology (BSG) standards framework 2014 (ref. 11 p. 8) states that “at least 80% of patients with an extra-hepatic stricture should have a stent sited and histology or cytology taken at first ERCP where the diagnosis is not already clear”. This audit seeks to determine the diagnostic yield of ERCP brush cytology in diagnosing pancreaticobiliary malignancies and its subsequent impact on patient management.
Methods
A retrospective analysis of data on ERCP brushings at Guy's and St. Thomas’ Hospital (GSTT) during the period 2008–2013 was carried out. Our audit population included any patient admitted at GSTT for ERCP from 2008 to 2013 (elective or as an inpatient). Data collection strategy encompassed three key aspects: (a) data were collected retrospectively between January and November 2014 for all patients who underwent ERCP; (b) ERCP procedure, clinical and demographic data were collected and analysed; and (c) data were obtained through the Department of Gastroenterology database, EndoSoft (Endosoft Leicester, UK), Department of Pathology database ‘Pathnet’ and Electronic Patient Records (EPRs) in order to conduct this audit. Where it was found that some of these patients had multiple ERCPs with brush cytology, the most recent cytology report was used. Data were checked with the Pathology Department to ensure its accuracy and identify any discrepancies. Once there was an established database of patients, an analysis of the EPRs for the outcome of cytology was carried out, essentially to see whether the brushing was reported as malignant/ suspicious of malignancy (grouped together for the purposes of this audit), equivocal or negative for malignancy. Of note, brush cytology included sending both the slides with samples on fixative solution and cutting of the whole brush.
Follow-up of each patient from the date of ERCP to November 2014 was carried out. Date of birth, gender and comorbidity data were also recorded. We analysed what investigations patients had before and after the ERCP to determine the influence of the cytology report on patient management. Subsequent tests included further imaging, endoscopy (eg, EUS), biopsies of suspicious lesions and tumour markers. We also noted the plan and prognosis for patients in cases where brushings were found to be malignant. Diagnoses were confirmed from the patient notes.
Results
Between 4 January 2008 and 27 December 2013, 162 patients underwent brush cytology. In each case, a stricture had been seen radiologically. 46.3% of patients were female, mean age 67.4 years. 65.4% of patients were subsequently diagnosed with malignancy, equal for male and female, and mean age 70.3 years.
Table 1 summarises the correlation between the final definite diagnoses and the earlier cytological diagnoses.
Validity analysis with cytology results
From the 162 patients included in our audit, 58 patients had positive cytology. Eight were found to have samples insufficient for cytology while eight patients had an equivocal cytology result. The sensitivity and specificity of brush cytology were 54.7% and 100.0%, respectively. The positive predictive value was 100.0%, and the negative predictive value was 53.85%.
Table 2 shows a summary of the results both with and without intention-to-treat analysis (which includes patients with an inadequate brushing sample for cytology and an equivocal cytology result).
Results with and without ITT analysis
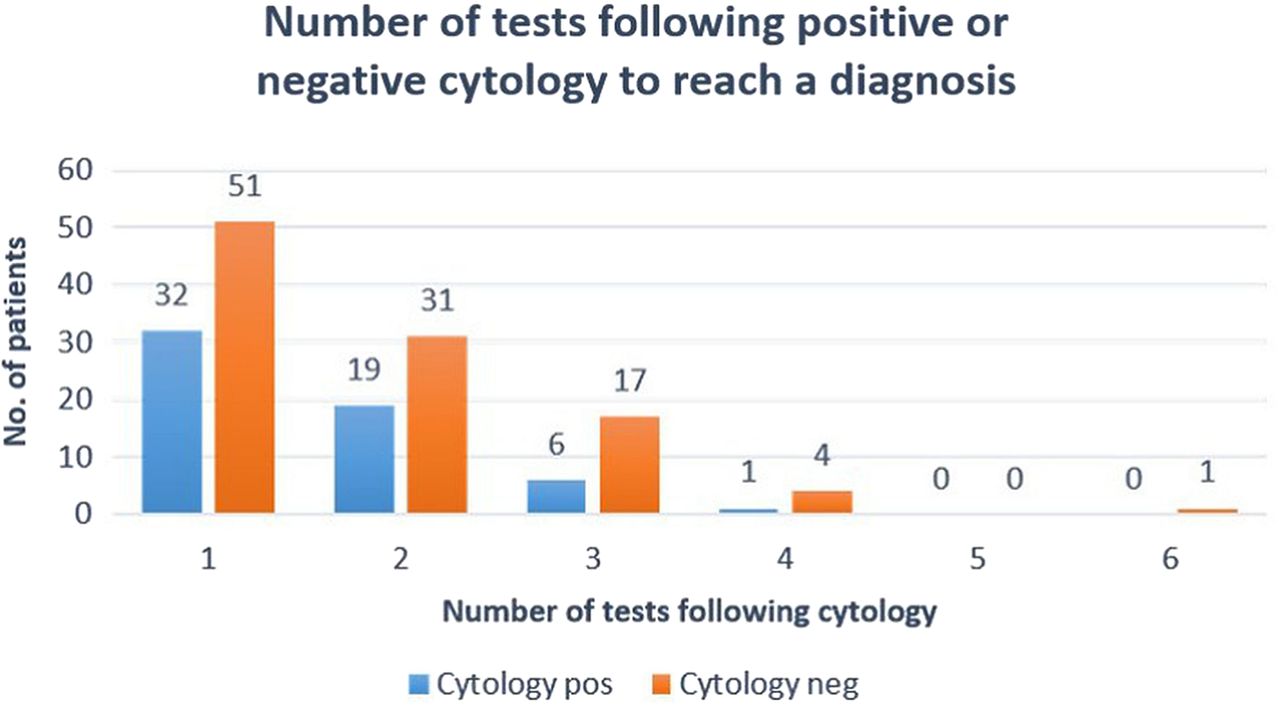
Figure 1 shows that fewer investigations were needed to reach a diagnosis following a positive cytology result from ERCP compared with a negative cytology result. The commonest tests done after ERCP were biopsies or fine needle aspiration of the suspected area in question either radiologically or by EUS.
{kind=link}
Number of further investigations needed following positive or negative cytology to reach a diagnosis.
Discussion
Much has been made of whether ERCP should be used in a therapeutic or diagnostic manner. Ohtsuka et al16 deemed ERCP adequate as the initial diagnostic modality for obtaining cytological confirmation with a particularly high yield of positive cytology from tumours in the head of pancreas. This supports the BSG Standards Framework 2014 recommendation that cytology should be taken where the diagnosis is not already clear.11
Burnett and Chokshi4 highlight the low sensitivity as a major flaw of ERCP brush cytology. The point is made that in cases with a high clinical suspicion of malignancy a negative cytology result is likely to be ignored. Also, in patients with resectable disease, a negative cytology result may not have bearing upon the intention for surgical intervention. In these cases, it seems the patient is put through an ERCP procedure without diagnostic gain, although they are often stented during the same ERCP procedure.4 Our study shows that patients with negative cytology were more likely to undergo further investigations than patients with positive cytology in cases where malignancy was suspected. Scudera et al17 also state that a positive cytological result may obviate the need for additional invasive diagnostic studies. Biopsies were the most frequent additional tests used in the present study. Three patients with negative cytology even went on to have a Whipple's procedure without any further investigations after the brush cytology. All three were found to have cancer. This confirms that a negative cytology result on its own should not be taken to mean absence of malignancy. The clinical picture is crucial. In cases of high clinical suspicion, negative results are further investigated. In this respect, an ERCP brush cytology procedure is no different from any other investigation.
A major problem identified by this audit is brushing extraction and preparation for cytology analysis. There were eight insufficient samples, which meant these could not be cytologically analysed by the pathology department. This accounted for 4.9% of our sample size. Differences in brushing technique or sample preparation by endoscopy assistants may explain some of these. It may be the case that better guidance is needed in these procedures to reduce the number of insufficient samples. Factors highlighted by the Department of Histopathology that contribute to an insufficient sample include the artefact from air drying that can occur if the brushing smear is not fixed in alcohol immediately and the reactive atypia resulting from the presence of a stent, which can give rise to equivocal reports. Previous studies have suggested a cytologist or a cytotechnician be present at the ERCP to prepare the sample real time; however, the financial feasibility and logistics for implementing this as standard practice may be considered unfavourable. Shieh et al18 showed that a stiffer brush design (infinity sampling device) increases diagnostic accuracy, likely due to increasing the number of cellular clusters obtained and consequently improving cellular yield. The development of newer techniques will improve bile duct sampling further. Ramchandani et al19 have shown that an accuracy of 82% can be obtained with the use of SpyBite on biopsies previously inconclusive using standard cytology brushings. Probe-based confocal laser endomicroscopy will allow for real-time histological evaluation.
On literature review, a number of studies have questioned how lesions suspicious of malignancy on cytological analysis should be managed. In our audit, we decided to include them with the confirmed cytological diagnoses of malignancy. Once again this calls for some overarching guidance and pathological input, for example, should the brushings be taken again at another ERCP if they cannot be confirmed to be malignant?
Our results are similar to those found in a larger review of 406 cases.3 Their overall reported diagnostic sensitivity and specificity were 59.8% and 98.1%, respectively. In a more recent study of 199 patients undergoing brush cytology, a diagnostic yield of 41%, sensitivity of 68% and specificity of 98% were reported.20 In considering various modalities in the field, a recent meta-analysis by Li et al21 showed that ERCP in combination with EUS was associated with a high diagnostic value for the detection of pancreatic malignancies compared with ERCP and EUS alone. This supports our view that ERCP should be used in conjunction with other modalities, and in fact it does play an important part in the diagnosis of malignancy.
Conclusion
Our audit is different from previous studies into the accuracy of brush cytology as we have explored the impact on patients where cytology is positive in reducing the number of further tests required to reach a diagnosis.
Our results for sensitivity and specificity of cytology brushings compare favourably with previous studies in the field. The development of guidance for the procedure would greatly benefit current practice by moving towards a more standardised process. In particular, further work on reducing the number of insufficient samples at brush cytology is needed to help improve the efficacy of the procedure.
The major benefit of an ERCP brush cytology procedure is a very high specificity—100% in this study. This, combined with the fact that an ERCP is simpler to execute, safer and cheaper than the available alternatives, gives the procedure a high diagnostic value. Even if it does not always negate the need for further investigations, it still provides useful diagnostic information.
Significance of this study
What is already known?
Sensitivities for brush cytology at ERCP are wide ranging (6% to 64%).
The increased availability of MRCP and EUS have questioned the need for ERCP and brush cytology.
ERCP carries with it a higher complication rate than other endoscopic procedures but allows for therapy such as stenting.
What this paper adds?
Our audit is of a large cohort where the sensitivity of brush cytology was high at 54.7%.
Where cytology is positive, patients undergo fewer further invasive investigations.
How might this impact on future clinical practice?
Sensitivities of cytology at ERCP should be improved further through stiffer brushes, SpyBite or real time pathology.
References
Footnotes
Contributors KS and RS performed the analysis and wrote the article jointly with BW. MW supervised the study and advised regarding the methodology. UM was the histologist who provided us with the histology reports. All authors contributed to refinement of the study protocol and approved the final manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.